Department of Medicine, University of Washington, Box 358061, 750 Republican St., Seattle, WA, 98109-4725, USA.
Centre de Santé de Ziguinchor, Ziguinchor, Senegal.
BMC Public Health. 2021 Mar 6;21(1):451. doi: 10.1186/s12889-021-10444-1.
Understanding the impact of food insecurity on HIV outcomes is critical for the development and implementation of effective, evidence-based interventions to address food insecurity and improve the HIV care cascade. We conducted a prospective, longitudinal study to determine the impact of food insecurity on HIV outcomes in Senegal, West Africa.
HIV-infected individuals presenting for care and initiation of ART through the Senegalese National AIDS program in Dakar and Ziguinchor were eligible for enrollment. Data were collected using interviews, clinical evaluations, laboratory analyses, and chart review at enrollment, month 6, and month 12. Logistic regression was used to determine the association between food insecurity and HIV outcomes.
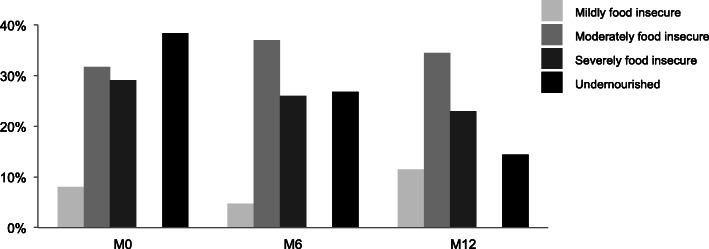
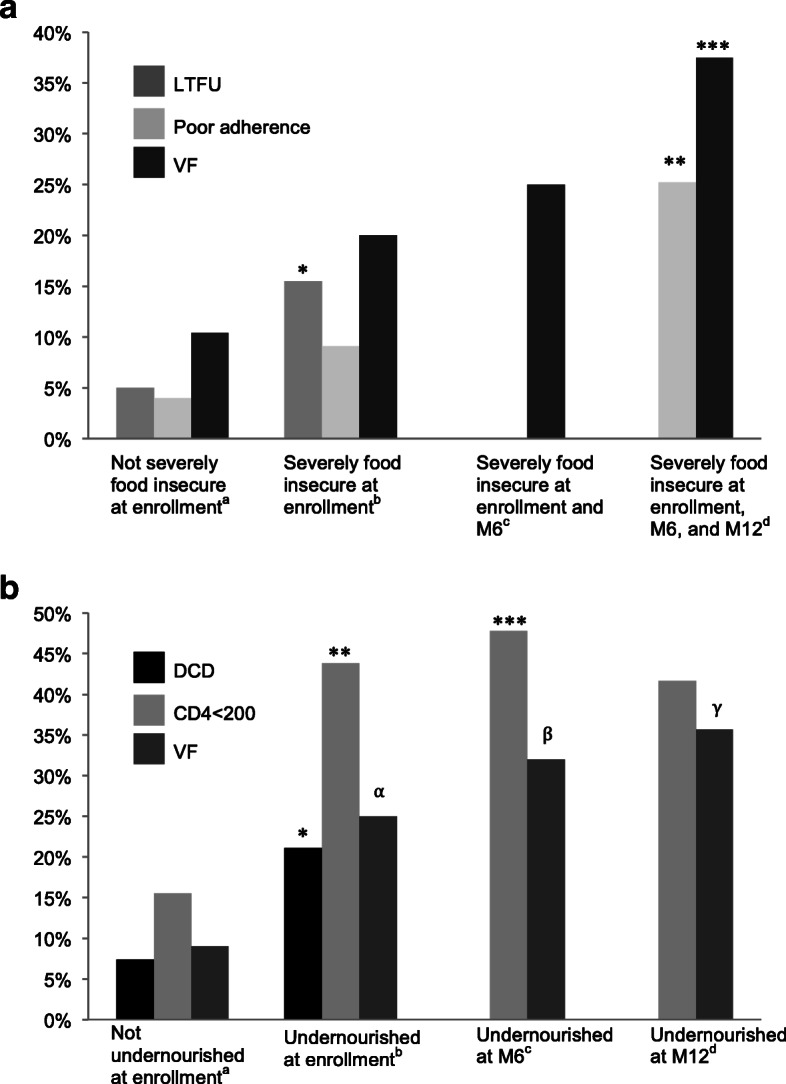
Among the 207 participants in this study, 70% were female and the median age was 37 years. The majority (69%) were food insecure at enrollment, 29% were severely food insecure, and 38% were undernourished. Nearly a third (32%) had no formal education, 23% practiced agriculture, and 40% owned livestock. The median daily food expenditure per person was $0.58. The median round trip transportation time to clinic was 90 min (IQR 30-240). The median cost of transportation to clinic was $1.74. At month 12, 69% were food insecure, 23% were severely food insecure, and 14% were undernourished. At month 12, 43% had not disclosed their HIV status; food insecurity was associated with non-disclosure of HIV-status due to fear of stigmatization and feelings of shame. Severe food insecurity was a strong predictor of loss to follow-up (OR 3.13 [1.08-9.06]) and persistent severe food insecurity was associated with virologic failure (OR 5.14 [1.01-26.29]) and poor adherence to ART 8.00 [1.11-57.57]. Poor nutritional status was associated with poor immunologic recovery (OR 4.24 [1.56-11.47]), virologic failure (OR 3.39 [1.13-10.21]), and death (OR 3.35 [1.40-8.03]).
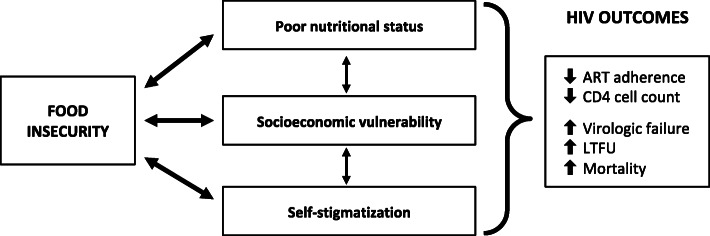
Severity and duration of food insecurity are important factors in understanding the relationship between food insecurity and HIV outcomes. Our findings highlight the importance of nutritional status, socioeconomic opportunity, and self-stigmatization in the complex pathway between food insecurity and HIV outcomes. Interdisciplinary, multisectoral efforts are needed to develop and implement effective interventions to address food insecurity among people living with HIV.
了解粮食不安全对艾滋病毒结果的影响对于制定和实施有效的循证干预措施以解决粮食不安全问题和改善艾滋病毒护理环节至关重要。我们在西非的塞内加尔进行了一项前瞻性、纵向研究,以确定粮食不安全对艾滋病毒结果的影响。
在达喀尔和济金绍尔通过塞内加尔国家艾滋病方案接受护理和开始接受抗逆转录病毒治疗的艾滋病毒感染者有资格入组。在入组时、第 6 个月和第 12 个月通过访谈、临床评估、实验室分析和病历回顾收集数据。使用逻辑回归来确定粮食不安全与艾滋病毒结果之间的关联。
在这项研究的 207 名参与者中,70%为女性,中位年龄为 37 岁。大多数(69%)在入组时粮食不安全,29%为严重粮食不安全,38%为营养不良。近三分之一(32%)没有受过正规教育,23%从事农业,40%拥有牲畜。人均每日食物支出中位数为 0.58 美元。往返诊所的中位交通时间为 90 分钟(IQR 30-240)。往返诊所的交通费用中位数为 1.74 美元。在第 12 个月时,69%的人粮食不安全,23%的人严重粮食不安全,14%的人营养不良。在第 12 个月时,43%的人没有透露他们的艾滋病毒状况;由于担心污名化和羞耻感,粮食不安全与艾滋病毒状况的不披露有关。严重粮食不安全是失访的强烈预测因素(OR 3.13[1.08-9.06]),持续严重粮食不安全与病毒学失败(OR 5.14[1.01-26.29])和抗逆转录病毒治疗的依从性差(OR 8.00[1.11-57.57])有关。营养不良状况与免疫恢复不良(OR 4.24[1.56-11.47])、病毒学失败(OR 3.39[1.13-10.21])和死亡(OR 3.35[1.40-8.03])有关。
粮食不安全的严重程度和持续时间是了解粮食不安全与艾滋病毒结果之间关系的重要因素。我们的研究结果强调了营养状况、社会经济机会和自我污名化在粮食不安全与艾滋病毒结果之间复杂途径中的重要性。需要采取跨学科、多部门的努力,制定和实施有效的干预措施,以解决艾滋病毒感染者的粮食不安全问题。