Ciccarone Center for the Prevention of Cardiovascular Disease, Division of Cardiology, Department of Medicine, Johns Hopkins Medical Institutions, Baltimore, MD, USA.
Department of Medicine, Section of Cardiology, Baylor College of Medicine, Houston, TX, USA.
Eur Heart J. 2021 Jun 1;42(21):2119-2129. doi: 10.1093/eurheartj/ehab111.
Whether isolated diastolic hypertension (IDH), as defined by the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) guideline, is associated with cardiovascular disease (CVD) has been disputed. We aimed to further study the associations of IDH with (i) subclinical CVD in the form of coronary artery calcium (CAC), (ii) incident systolic hypertension, and (iii) CVD events.
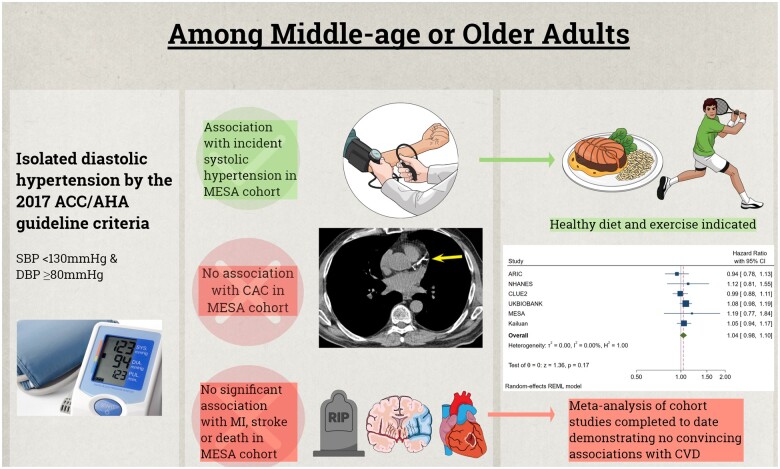
We used multivariable-adjusted logistic and Cox regression to test whether IDH by 2017 ACC/AHA criteria (i.e. systolic blood pressure <130 mmHg and diastolic blood pressure ≥80 mmHg) was associated with the above outcomes in the Multi-Ethnic Study of Atherosclerosis (MESA). In a random-effects meta-analysis of the association between IDH and CVD events, we combined the MESA results with those from seven other previously published cohort studies. Among the 5104 MESA participants studied, 7.5% had IDH by the 2017 ACC/AHA criteria. There was no association between IDH and CAC [e.g. adjusted prevalence odds ratio for CAC >0 of 0.88 (95% CI 0.66, 1.17)]. Similarly, while IDH was associated with incident systolic hypertension, there was no statistically significant associations with incident CVD [hazard ratio 1.19 (95% CI 0.77, 1.84)] or death [hazard ratio 0.94 (95% CI 0.65, 1.36)] over 13 years in MESA. In a stratified meta-analysis of eight cohort studies (10 037 843 participants), the 2017 IDH definition was also not consistently associated with CVD and the relative magnitude of any potential association was noted to be numerically small [e.g. depending on inclusion criteria applied in the stratification, the adjusted hazard ratios ranged from 1.04 (95% CI 0.98, 1.10) to 1.09 (95% 1.03, 1.15)].
The lack of consistent excess in CAC or CVD suggests that emphasis on healthy lifestyle rather than drug therapy is sufficient among the millions of middle-aged or older adults who now meet the 2017 ACC/AHA criteria for IDH, though they require follow-up for incident systolic hypertension. These findings may not extrapolate to adults younger than 40 years, motivating further study in this age group.
根据 2017 年美国心脏病学会(ACC)/美国心脏协会(AHA)指南定义的孤立性舒张期高血压(IDH)是否与心血管疾病(CVD)有关存在争议。我们旨在进一步研究 IDH 与(i)冠状动脉钙(CAC)形式的亚临床 CVD,(ii)新发收缩期高血压和(iii)CVD 事件的关联。
我们使用多变量调整的逻辑和 Cox 回归来检验 2017 年 ACC/AHA 标准(即收缩压<130mmHg 且舒张压≥80mmHg)是否与动脉粥样硬化多民族研究(MESA)中的上述结果相关。在一项 IDH 与 CVD 事件关联的随机效应荟萃分析中,我们将 MESA 的结果与之前发表的七项其他队列研究的结果结合在一起。在研究的 5104 名 MESA 参与者中,有 7.5% 符合 2017 年 ACC/AHA 标准的 IDH。IDH 与 CAC 之间没有关联[例如 CAC>0 的调整患病率比值比为 0.88(95%CI 0.66,1.17)]。同样,虽然 IDH 与新发收缩期高血压相关,但在 MESA 中,在 13 年内与新发 CVD[危险比 1.19(95%CI 0.77,1.84)]或死亡[危险比 0.94(95%CI 0.65,1.36)]之间没有统计学意义的关联。在对八项队列研究(10037843 名参与者)的分层荟萃分析中,2017 年 IDH 定义也与 CVD 不一致,并且注意到任何潜在关联的相对幅度在数值上较小[例如,根据分层中应用的纳入标准,调整后的危险比范围为 1.04(95%CI 0.98,1.10)至 1.09(95%CI 1.03,1.15)]。
缺乏 CAC 或 CVD 的一致增加表明,对于现在符合 2017 年 ACC/AHA IDH 标准的数百万名中年或老年成年人,强调健康的生活方式而不是药物治疗就足够了,尽管他们需要监测新发收缩期高血压。这些发现可能不适用于 40 岁以下的成年人,这促使在该年龄组进一步研究。