University of Colorado Anschutz Medical Campus, Aurora, CO, USA, School of Public Health, Department of Health Systems, Management, and Policy (D.R.F., C.B., R.C.L.).
Department of Biostatistics and Informatics (G.K.G.).
Circ Cardiovasc Qual Outcomes. 2021 Mar;14(3):e006572. doi: 10.1161/CIRCOUTCOMES.120.006572. Epub 2021 Mar 8.
Although cardiac rehabilitation (CR) is a Class I Guideline recommendation, and has been shown to be a cost-effective intervention after a cardiac event, it has been reimbursed at levels insufficient to cover hospital operating costs. In January 2011, Medicare increased payment for CR in hospital outpatient settings by ≈180%. We evaluated the association between this payment increase and participation in CR of eligible Medicare beneficiaries to better understand the relationship between reimbursement policy and CR utilization.
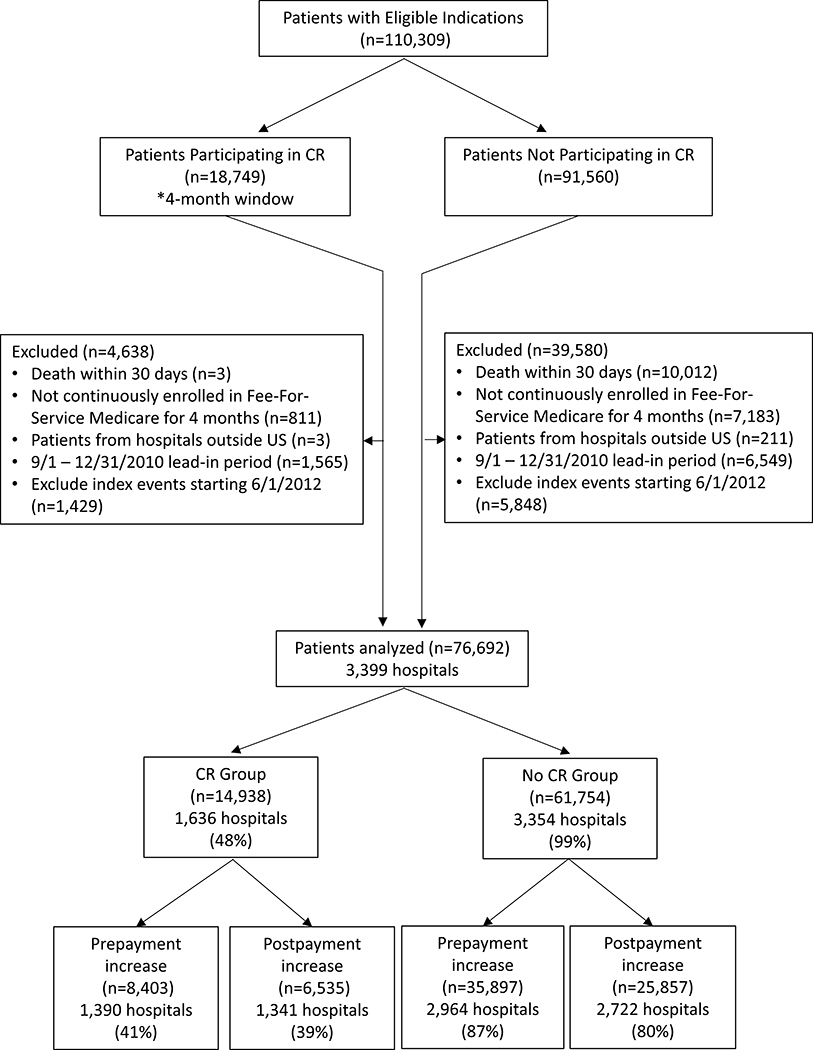
From a 5% Medicare claims sample, we identified patients with acute myocardial infarction, coronary artery bypass surgery, percutaneous coronary intervention, or cardiac valve surgery between January 1, 2009 and September 30, 2012, alive 30 days after their event, with continuous enrollment in Medicare fee-for-service, Part A/B for 4 months. Trends and changes in CR participation were estimated using an interrupted time series approach with a hierarchical logistic model, hospital random intercepts, adjusted for patient, hospital, market, and seasonality factors. Estimates were expressed using average marginal effects on a percent scale.
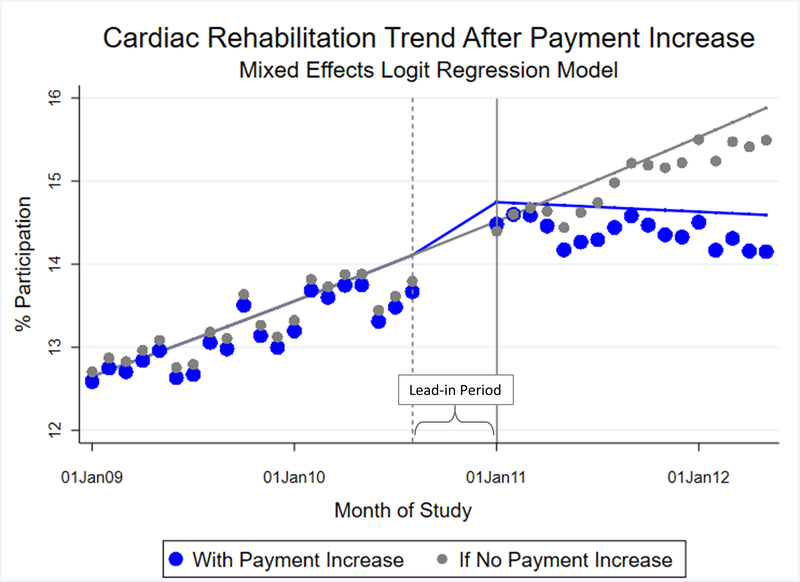
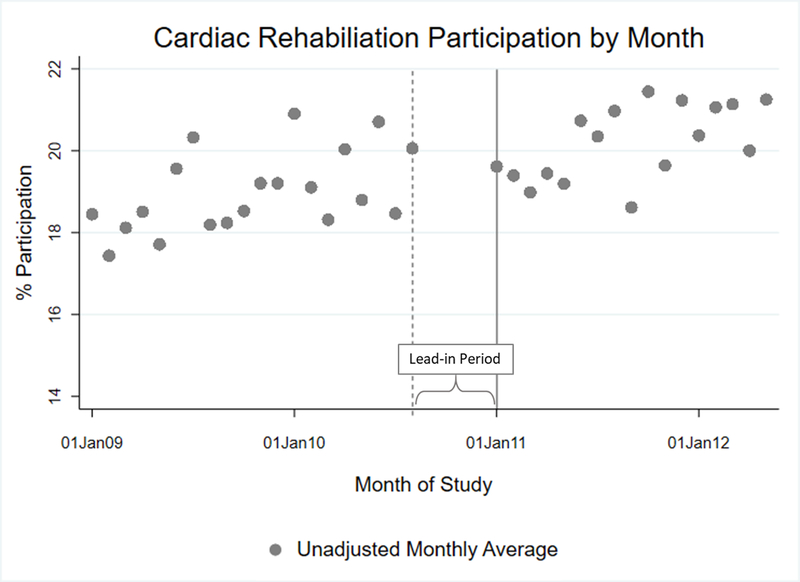
Among 76 695 eligible patients, average annual CR participation was 19.5% overall. In the period before payment increase, adjusted annual participation grew by 1.1 percentage points (95% CI, 0.48-2.4). No immediate change occurred in CR participation when the new payment was implemented. In the period after payment increase, on average, 20% of patients participated in CR annually. The annual growth rate in CR participation slowed in the post-period by 1.3 percentage points (95% CI, -2.4 to -0.12) compared with the prior period. Results were somewhat sensitive to time window variations.
The 2011 increase in Medicare reimbursement for CR was not associated with an increase in participation. Future studies should evaluate whether payment did not reach a threshold to incentivize hospitals or if hospitals were not sensitive to reimbursement changes.
尽管心脏康复(CR)是 I 类指南推荐的治疗方法,并且已被证明是心脏事件后的一种具有成本效益的干预措施,但它的报销水平还不足以覆盖医院的运营成本。2011 年 1 月,医疗保险(Medicare)将医院门诊环境下的 CR 支付增加了约 180%。我们评估了此次支付增加与符合条件的 Medicare 受益人的 CR 参与之间的关联,以更好地了解报销政策与 CR 使用之间的关系。
我们从 Medicare 索赔的 5%样本中,确定了在 2009 年 1 月 1 日至 2012 年 9 月 30 日期间患有急性心肌梗死、冠状动脉旁路移植术、经皮冠状动脉介入治疗或心脏瓣膜手术的患者,在发病后 30 天存活,并且连续参加 Medicare 按服务收费、A 部分/B 部分的 4 个月。使用具有分层逻辑模型、医院随机截距的中断时间序列方法来估计 CR 参与率的趋势和变化,调整了患者、医院、市场和季节性因素。使用百分比的平均边际效应表示估计值。
在 76695 名符合条件的患者中,总体上每年的 CR 参与率为 19.5%。在支付增加之前的时期,调整后的年度参与率增长了 1.1 个百分点(95%置信区间,0.48-2.4)。新支付实施后,CR 参与率没有立即发生变化。在支付增加后的时期,平均每年有 20%的患者参与 CR。与前一时期相比,后一时期 CR 参与率的年增长率下降了 1.3 个百分点(95%置信区间,-2.4 至-0.12)。结果对时间窗口变化有些敏感。
2011 年 Medicare 对 CR 的报销增加与参与率的增加无关。未来的研究应该评估支付是否没有达到激励医院的门槛,或者医院是否对报销变化不敏感。