Section of Cardiovascular Medicine, Department of Internal Medicine, Yale School of Medicine, New Haven, Connecticut.
Department of Health Policy and Management, Yale School of Public Health, New Haven, Connecticut.
JAMA Netw Open. 2019 Mar 1;2(3):e191938. doi: 10.1001/jamanetworkopen.2019.1938.
Medicare and other organizations have focused on improving quality of care for patients with acute myocardial infarction (AMI) over the last 2 decades. However, there is no comprehensive perspective on the evolution of outcomes for AMI during that period, and it is unknown whether temporal changes varied by patient subgroup, hospital, or county.
To provide a comprehensive evaluation of national trends in inpatient outcomes and costs of AMI during this period.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included analysis of data from a sample of 4 367 485 Medicare fee-for-service beneficiaries aged 65 years or older from January 1, 1995, through December 31, 2014, across 5680 hospitals in the United States. Analyses were conducted from January 15 to June 5, 2018.
Thirty-day all-cause mortality at the patient, hospital, and county levels. Additional outcomes included 30-day all-cause readmissions; 1-year recurrent AMI; in-hospital mortality; length of hospital stay; 2014 Consumer Price Index-adjusted median Medicare inpatient payment per AMI discharge; and rates of catheterization, percutaneous coronary intervention, and coronary artery bypass graft surgery.
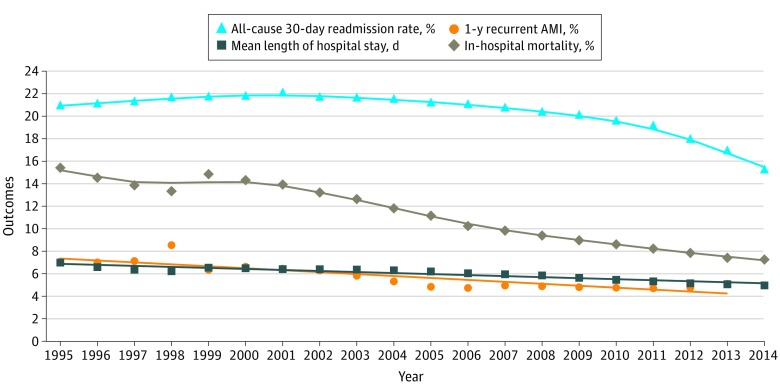
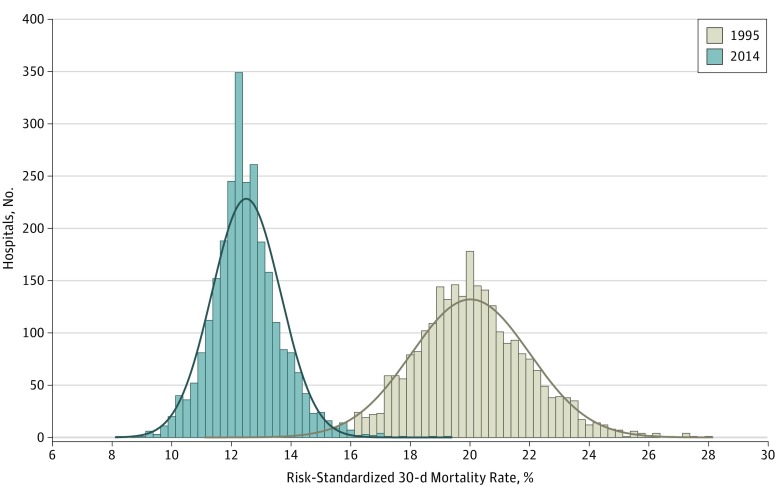
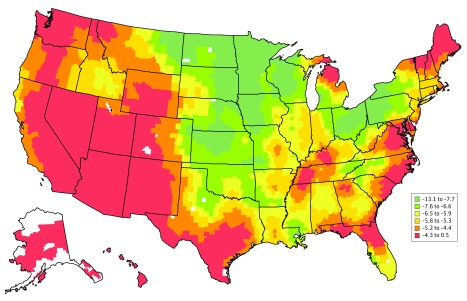
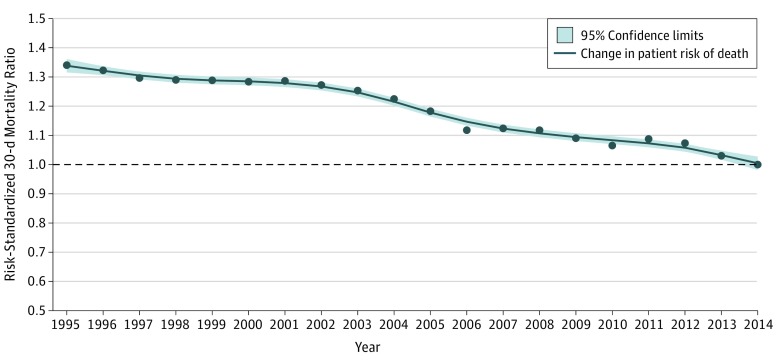
The cohort included 4 367 485 Medicare fee-for-service patients aged 65 years or older hospitalized for AMI during the study period. Between 1995 and 2014, the mean (SD) age of patients increased from 76.9 (7.2) to 78.2 (8.7) years, the percentage of female patients declined from 49.5% to 46.1%, the percentage of white patients declined from 91.0% to 86.2%, and the percentage of black patients increased from 5.9% to 8.0%. There were declines in AMI hospitalizations (914 to 566 per 100 000 beneficiary-years); 30-day mortality (20.0% to 12.4%; difference, 7.6 percentage points; 95% CI, 7.3-7.8 percentage points); 30-day all-cause readmissions (21.0% to 15.3%; difference, 5.7 percentage points; 95% CI, 5.4-6.0 percentage points); and 1-year recurrent AMI (7.1% to 5.1%; difference, 2.0 percentage points; 95% CI, 1.8-2.2 percentage points). There were increases in the 2014 Consumer Price Index-adjusted median (interquartile range) Medicare inpatient payment per AMI discharge ($9282 [$6969-$12 173] to $11 031 [$8099-$16 861]); 30-day inpatient catheterization (44.2% to 59.9%; difference, 15.7 percentage points; 95% CI, 15.4-16.0 percentage points); and inpatient percutaneous coronary intervention (18.8% to 43.3%; difference, 24.5 percentage points; 95% CI, 24.2-24.7 percentage points). Coronary artery bypass graft surgery rates decreased from 14.4% to 10.2% (difference, 4.2 percentage points; 95% CI, 3.9-4.3 percentage points). There was heterogeneity by hospital and county in the mortality changes over time.
This study shows marked improvements in short-term mortality and readmissions, with an increase in in-hospital procedures and payments, for the increasingly smaller number of Medicare beneficiaries with AMI.
在过去的 20 年中,医疗保险和其他组织一直致力于改善急性心肌梗死(AMI)患者的护理质量。然而,在此期间,AMI 患者结局的演变情况尚缺乏全面的视角,而且尚不清楚时间变化是否因患者亚组、医院或县而异。
提供在此期间 AMI 患者住院结局和费用的全国趋势的综合评估。
设计、地点和参与者:本队列研究分析了来自美国 5680 家医院的 4367485 名 65 岁或以上的 Medicare 按服务收费受益人的样本数据,这些患者于 1995 年 1 月 1 日至 2014 年 12 月 31 日期间因 AMI 住院。分析于 2018 年 1 月 15 日至 6 月 5 日进行。
患者、医院和县级 30 天全因死亡率。其他结局包括 30 天全因再入院;1 年复发 AMI;住院期间死亡率;住院时间;2014 年消费者价格指数调整后每例 AMI 出院的 Medicare 住院支付中位数;以及经导管检查、经皮冠状动脉介入治疗和冠状动脉旁路移植术的比例。
该队列包括在研究期间因 AMI 住院的 4367485 名 Medicare 按服务收费的 65 岁或以上的患者。1995 年至 2014 年间,患者的平均(SD)年龄从 76.9(7.2)岁增至 78.2(8.7)岁,女性患者的比例从 49.5%降至 46.1%,白人患者的比例从 91.0%降至 86.2%,黑人患者的比例从 5.9%增至 8.0%。AMI 住院人数(每 10 万受益人的年住院率从 914 降至 566);30 天死亡率(从 20.0%降至 12.4%;差异,7.6 个百分点;95%CI,7.3-7.8 个百分点);30 天全因再入院率(从 21.0%降至 15.3%;差异,5.7 个百分点;95%CI,5.4-6.0 个百分点);以及 1 年复发 AMI(从 7.1%降至 5.1%;差异,2.0 个百分点;95%CI,1.8-2.2 个百分点)。2014 年消费者价格指数调整后每例 AMI 出院的 Medicare 住院支付中位数(四分位距)有所增加(从 9282 美元[6969-12173 美元]增至 11031 美元[8099-16861 美元]);30 天内住院经导管检查(从 44.2%增至 59.9%;差异,15.7 个百分点;95%CI,15.4-16.0 个百分点);以及住院经皮冠状动脉介入治疗(从 18.8%增至 43.3%;差异,24.5 个百分点;95%CI,24.2-24.7 个百分点)。冠状动脉旁路移植术的比例从 14.4%降至 10.2%(差异,4.2 个百分点;95%CI,3.9-4.3 个百分点)。死亡率随时间变化的变化在医院和县级存在差异。
本研究表明,对于越来越少的 Medicare 急性心肌梗死患者,短期死亡率和再入院率显著改善,住院治疗和支付的程序和费用增加。