Streese Lukas, Vaes Anja, Infanger Denis, Roth Ralf, Hanssen Henner
Department of Sport, Exercise and Health, University of Basel, Basel, Switzerland.
Front Physiol. 2021 Feb 18;12:608985. doi: 10.3389/fphys.2021.608985. eCollection 2021.
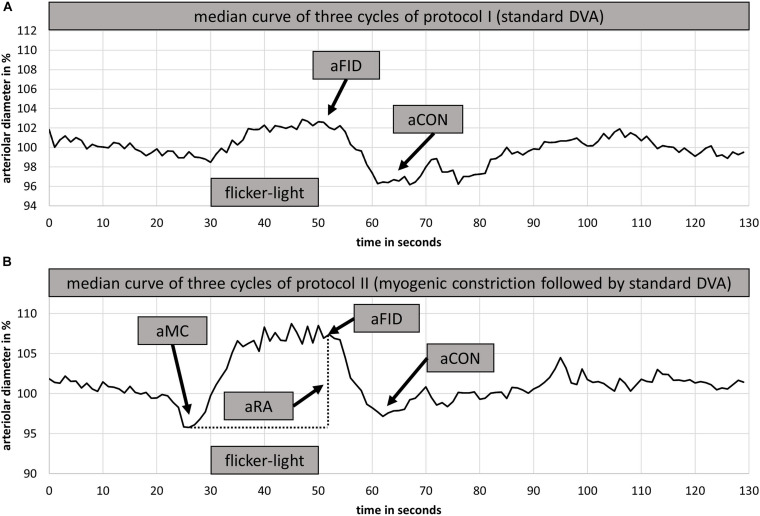
BACKGROUND/AIMS: Flicker-light induced retinal vessel dilatation (FID), a marker of microvascular endothelial function, has been shown to be blunted in sedentary cardiovascular risk patients (SR) as well as healthy physically active individuals (HA). This study aimed to quantify the retinal myogenic response to blood pressure (BP) peaks and its effects on consecutive FID for differentiation of microvascular health.
Ten HA and eleven SR with a previously established restriction of arteriolar FID (aFID) (<2.2%) were invited in order to assess BP-induced myogenic constriction following a standardized handgrip task and a consecutive FID. BP was measured beat-to-beat.
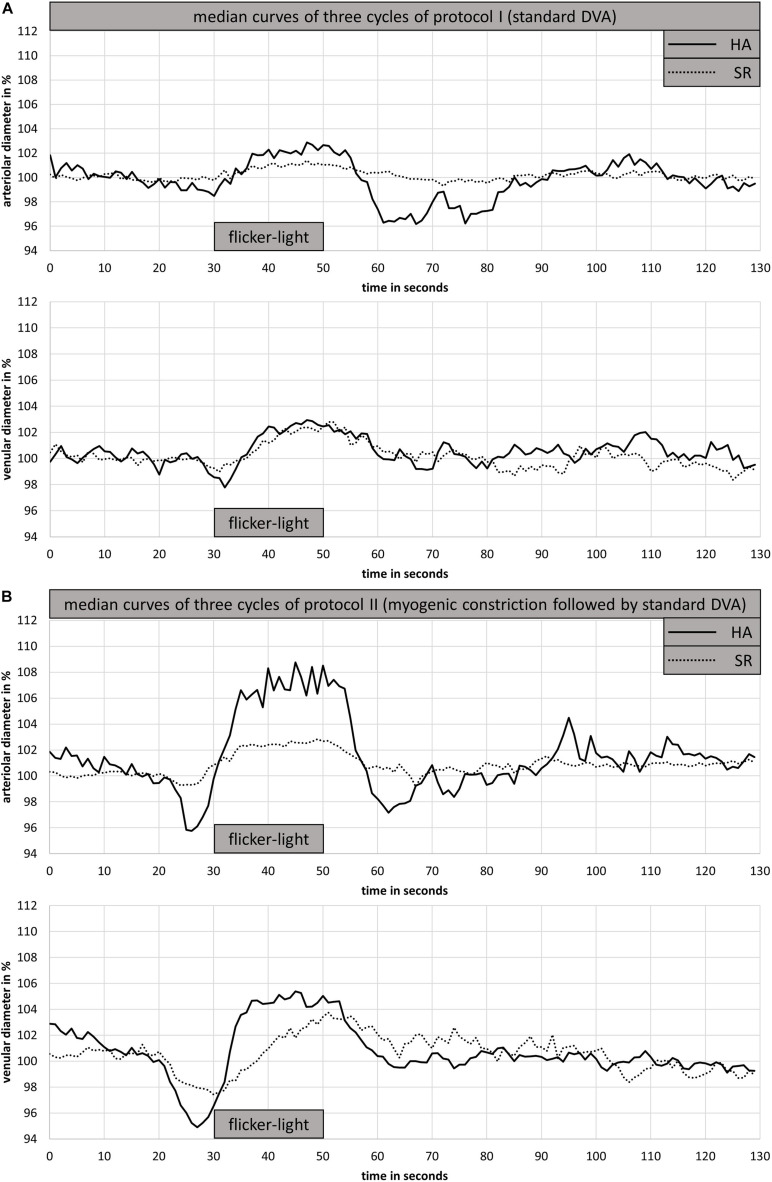
The complete dataset of nine HA (3 female, mean age 65 years) and nine SR (5 female, mean age 61 years) individuals was analyzed. The central retinal arteriolar diameter equivalent (CRAE) was 183 ± 11 μm for HA and 176 ± 20 μm for SR. Initial baseline aFID was 1.6 ± 0.4% in HA and 1.6 ± 0.7% in SR. Systolic ( = 0.334) and diastolic ( = 0.245) BP increase following the handgrip task was in the range of 20-30% and comparable in both groups. BP increase was followed by a significantly higher arteriolar (-2.9 ± 1.3% vs. -1.3 ± 0.6%, < 0.01) myogenic constriction in HA compared to SR. Moreover, in the consecutive assessment of FID directly after the BP-induced vessel constriction, aFID (4.1 ± 2.0% vs. 1.6 ± 0.9%, < 0.01) was higher in HA compared to SR.
Initial baseline aFID was blunted in HA and SR. Retinal myogenic constriction was impaired in SR compared to HA. The consecutive aFID after BP-induced myogenic constriction recovered in HA but remained blunted in SR. Additional assessment of retinal myogenic constriction needs to be considered to improve CV risk stratification and reduce false-positive findings of endothelial dysfunction in otherwise healthy active individuals.
ClinicalTrials.gov: NCT03986892 (https://clinicaltrials.gov/ct2/show/NCT03986892).
背景/目的:闪烁光诱导的视网膜血管扩张(FID)是微血管内皮功能的一个标志物,已被证明在久坐的心血管风险患者(SR)以及健康的体力活动个体(HA)中会减弱。本研究旨在量化视网膜对血压(BP)峰值的肌源性反应及其对连续FID的影响,以区分微血管健康状况。
邀请了10名HA和11名先前已确定存在小动脉FID(aFID)受限(<2.2%)的SR,以便在标准化握力任务及随后的FID后评估血压诱导的肌源性收缩。逐搏测量血压。
分析了9名HA(3名女性,平均年龄65岁)和9名SR(5名女性,平均年龄61岁)个体的完整数据集。HA的视网膜中央小动脉直径等效值(CRAE)为183±11μm,SR为176±20μm。HA的初始基线aFID为1.6±0.4%,SR为1.6±0.7%。握力任务后收缩压(=0.334)和舒张压(=0.245)升高幅度在20 - 30%范围内,两组相当。与SR相比,HA在血压升高后小动脉肌源性收缩明显更高(-2.9±1.3%对-1.3±0.6%,<0.01)。此外,在血压诱导血管收缩后直接进行的FID连续评估中,HA的aFID(4.1±2.0%对1.6±0.9%,<0.01)高于SR。
HA和SR的初始基线aFID均减弱。与HA相比,SR的视网膜肌源性收缩受损。血压诱导的肌源性收缩后连续的aFID在HA中恢复,但在SR中仍减弱。需要考虑额外评估视网膜肌源性收缩,以改善心血管风险分层并减少在其他方面健康的活跃个体中内皮功能障碍的假阳性结果。
ClinicalTrials.gov:NCT03986892(https://clinicaltrials.gov/ct2/show/NCT03986892)。