Gao Xingxing, Huang Hechen, Wang Yubo, Pan Caixu, Yin Shengyong, Zhou Lin, Zheng Shusen
Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China.
NHC Key Laboratory of Combined Multi-organ Transplantation, Hangzhou, China.
Front Oncol. 2021 Feb 19;10:610513. doi: 10.3389/fonc.2020.610513. eCollection 2020.
The tumor microenvironment (TME) plays a critical role in the pathogenesis of hepatocellular carcinoma (HCC). However, underlying compositions and functions that drive the establishment and maintenance of the TME classifications are less-well understood.
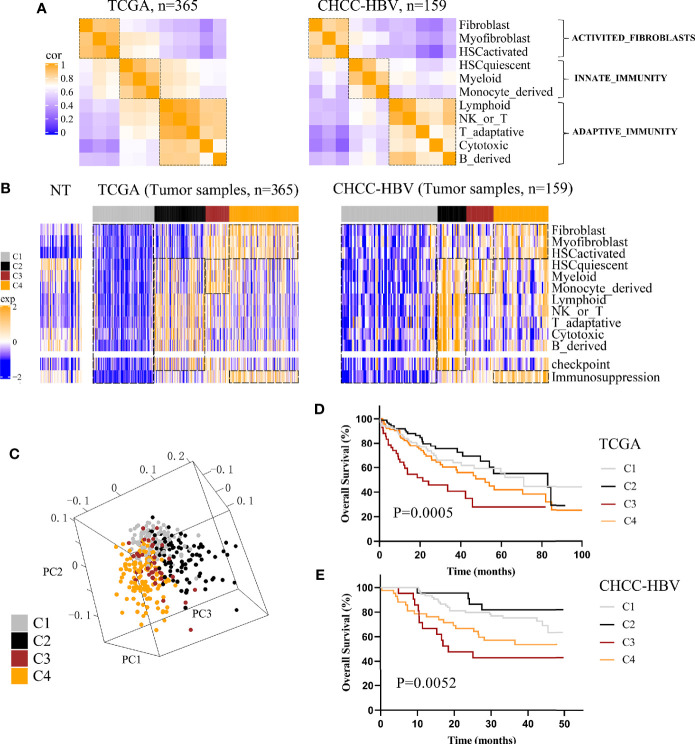
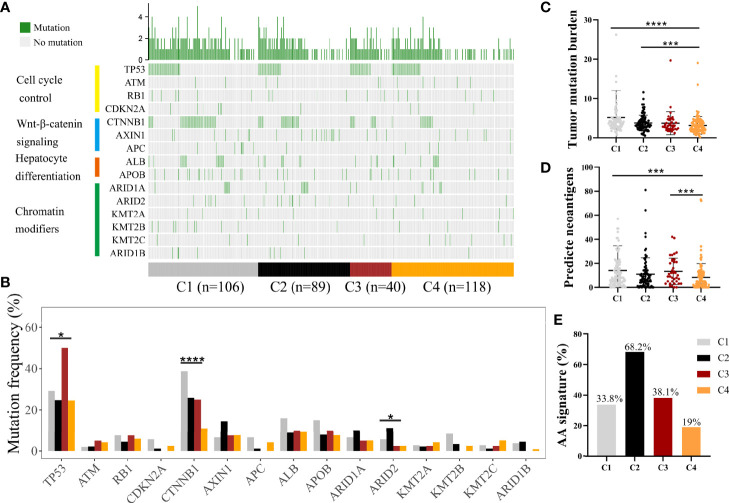
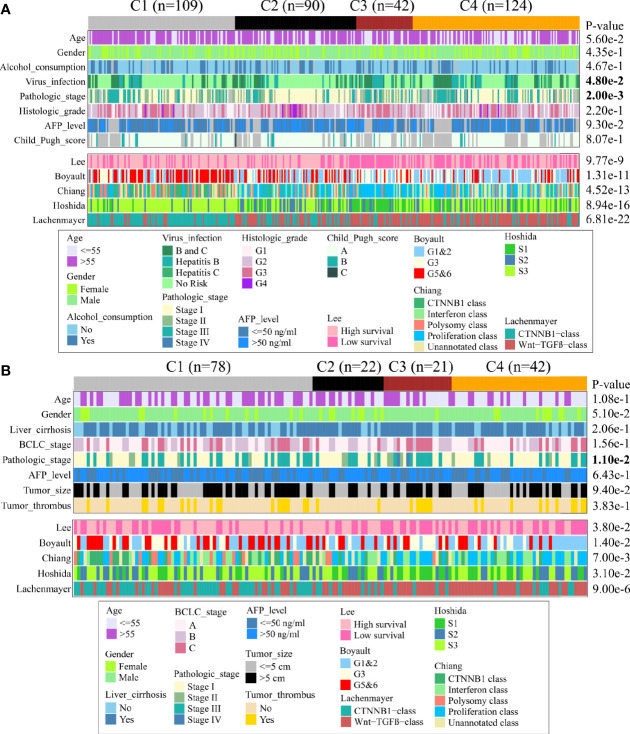
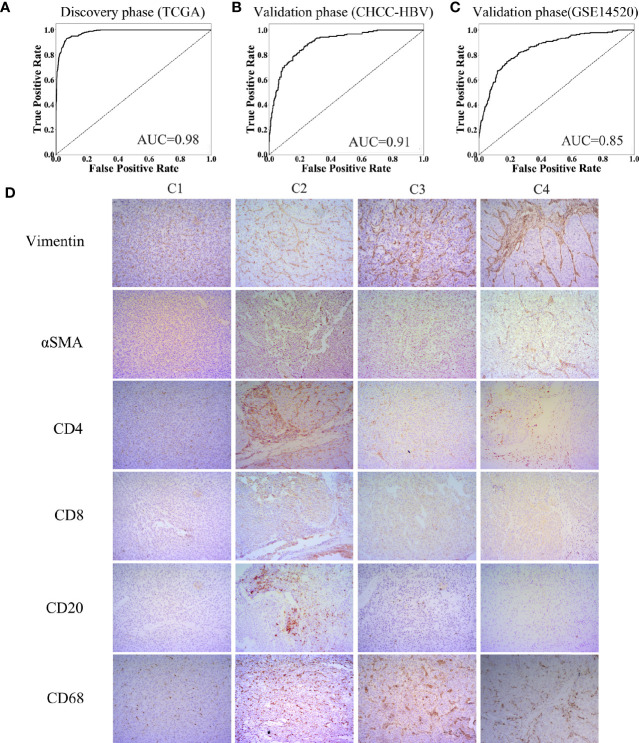
A total of 766 HCC patients from three public cohorts were clustered into four immune-related subclasses based on 13 TME signatures (11 immune-related cells and 2 immune-related pathways) calculated by MCP-counter. After analyzing the landscapes of functional annotation, methylation, somatic mutation, and clinical characteristics, we built a TME-based Support Vector Machine of 365 patients (discovery phase) and 401 patients (validation phase). We applied this SVM model on another two independent cohorts of patients who received sorafenib/pembrolizumab treatment.
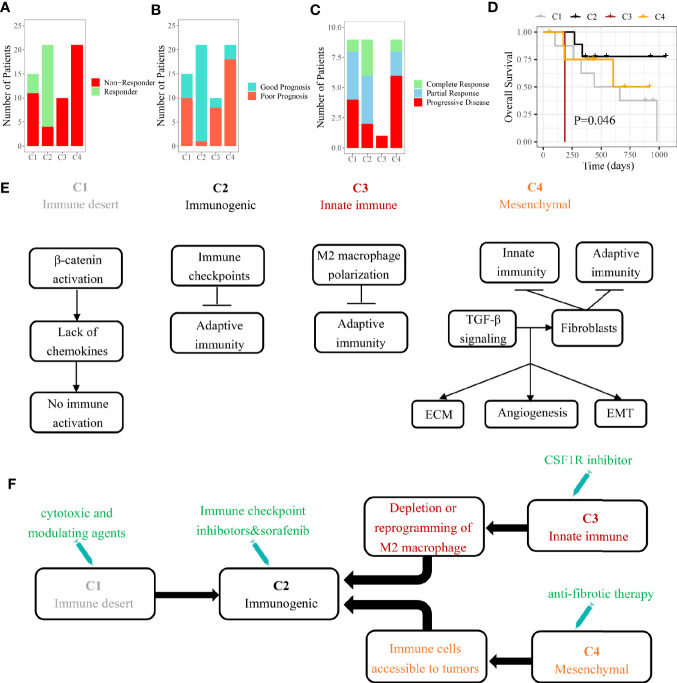
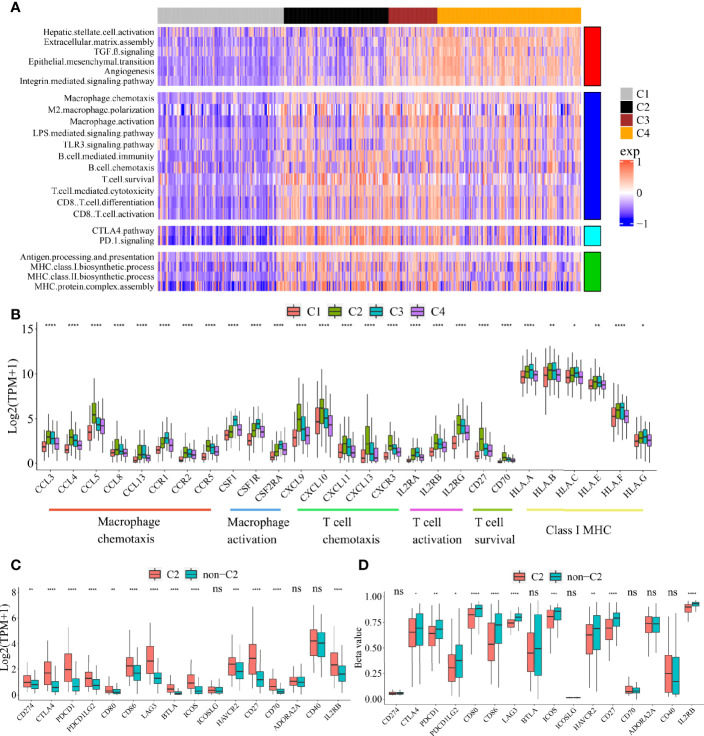
About 33% of patients displayed an immune desert pattern. The other subclasses were different in abundance of tumor infiltrating cells. The Immunogenic subclass (17%) associated with the best prognosis presented a massive T cell infiltration and an activation of immune checkpoint pathway. The 13 TME signatures showed a good potential to predict the TME classification (average AUC = 88%). Molecular characteristics of immunohistochemistry from Zhejiang cohort supported our SVM classification. The optimum response to pembrolizumab (78%) and sorafenib (81%) was observed in patients belonging to the Immunogenic subclass.
The HCC patients from distinct immune subclass showed significant differences in clinical prognosis and response to personalized treatment. Based on tumor transcriptome data, our workflow can help to predict the clinical outcomes and to find appropriate treatment strategies for HCC patients.
肿瘤微环境(TME)在肝细胞癌(HCC)的发病机制中起关键作用。然而,驱动TME分类的建立和维持的潜在组成和功能尚不清楚。
基于MCP-counter计算的13个TME特征(11种免疫相关细胞和2种免疫相关途径),将来自三个公共队列的766例HCC患者聚类为四个免疫相关亚类。在分析功能注释、甲基化、体细胞突变和临床特征的情况后,我们构建了一个基于TME的支持向量机,其中发现阶段有365例患者,验证阶段有401例患者。我们将这个支持向量机模型应用于另外两个接受索拉非尼/派姆单抗治疗的独立患者队列。
约33%的患者表现出免疫荒漠模式。其他亚类在肿瘤浸润细胞的丰度上有所不同。与最佳预后相关的免疫原性亚类(17%)表现出大量T细胞浸润和免疫检查点途径的激活。这13个TME特征显示出良好的预测TME分类的潜力(平均AUC = 88%)。浙江队列的免疫组织化学分子特征支持我们的支持向量机分类。在属于免疫原性亚类的患者中观察到对派姆单抗(78%)和索拉非尼(81%)的最佳反应。
来自不同免疫亚类的HCC患者在临床预后和对个性化治疗的反应方面存在显著差异。基于肿瘤转录组数据,我们的工作流程有助于预测HCC患者的临床结局并找到合适的治疗策略。