D'Amato Daphne, De Vincentis Antonio, Malinverno Federica, Viganò Mauro, Alvaro Domenico, Pompili Maurizio, Picciotto Antonino, Palitti Valeria Pace, Russello Maurizio, Storato Silvia, Pigozzi Marie Graciella, Calvaruso Vincenza, De Gasperi Elisabetta, Lleo Ana, Castellaneta Antonino, Pellicelli Adriano, Cazzagon Nora, Floreani Annarosa, Muratori Luigi, Fagiuoli Stefano, Niro Grazia Anna, Feletti Valentina, Cozzolongo Raffaele, Terreni Natalia, Marzioni Marco, Pellicano Rinaldo, Pozzoni Pietro, Baiocchi Leonardo, Chessa Luchino, Rosina Floriano, Bertino Gaetano, Vinci Maria, Morgando Anna, Vanni Ester, Scifo Gaetano, Sacco Rodolfo, D'Antò Maria, Bellia Valentina, Boldizzoni Roberto, Casella Silvia, Omazzi Barbara, Poggi Guido, Cristoferi Laura, Gerussi Alessio, Ronca Vincenzo, Venere Rosanna, Ponziani Francesca, Cannavò Maria, Mussetto Alessandro, Fontana Rosanna, Losito Francesco, Frazzetto Evelise, Distefano Marco, Colapietro Francesca, Labanca Sara, Marconi Giulia, Grassi Giuseppe, Galati Giovanni, O'Donnell Sarah Elizabeth, Mancuso Clara, Mulinacci Giacomo, Palermo Andrea, Claar Ernesto, Izzi Antonio, Picardi Antonio, Invernizzi Pietro, Carbone Marco, Vespasiani-Gentilucci Umberto
Division of Gastroenterology, Centre for Autoimmune Liver Diseases, Department of Medicine and Surgery, University of Milano-Bicocca, European Reference Network on Hepatological Diseases (ERN RARE-LIVER), San Gerardo Hospital, Monza, Italy.
Internal Medicine and Hepatology, University Campus Bio-Medico of Rome, Rome, Italy.
JHEP Rep. 2021 Jan 27;3(2):100248. doi: 10.1016/j.jhepr.2021.100248. eCollection 2021 Apr.
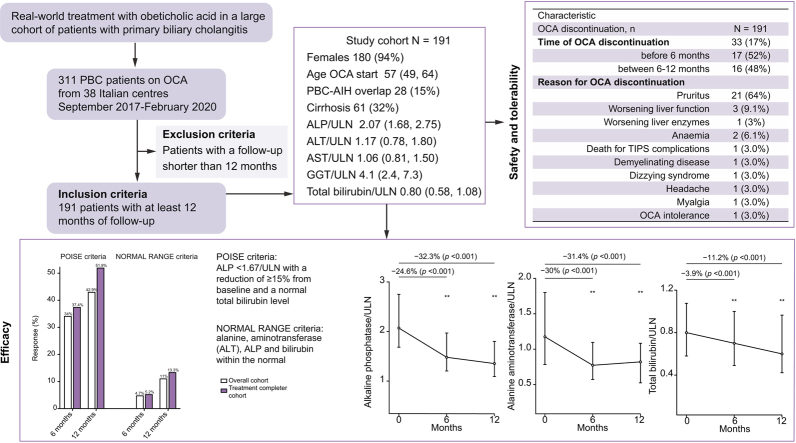
BACKGROUND & AIMS: Obeticholic acid (OCA) is the second-line treatment approved for patients with primary biliary cholangitis (PBC) and an inadequate response or intolerance to ursodeoxycholic acid. We aimed to evaluate the effectiveness and safety of OCA under real-world conditions.
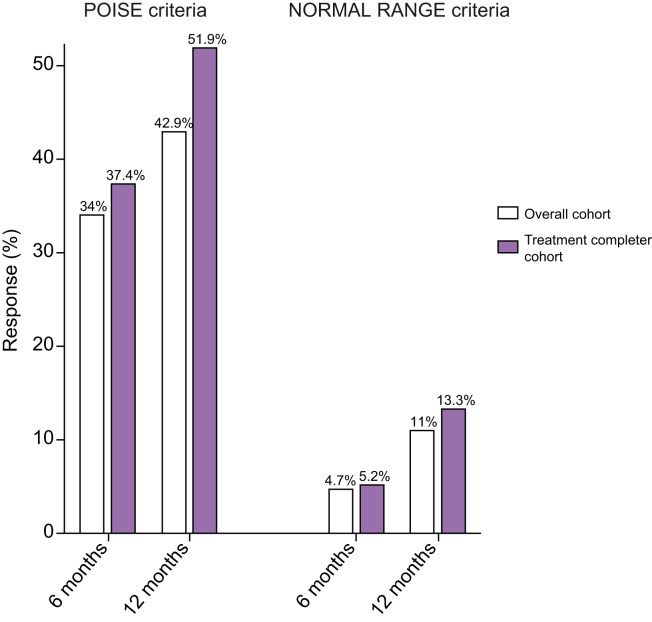
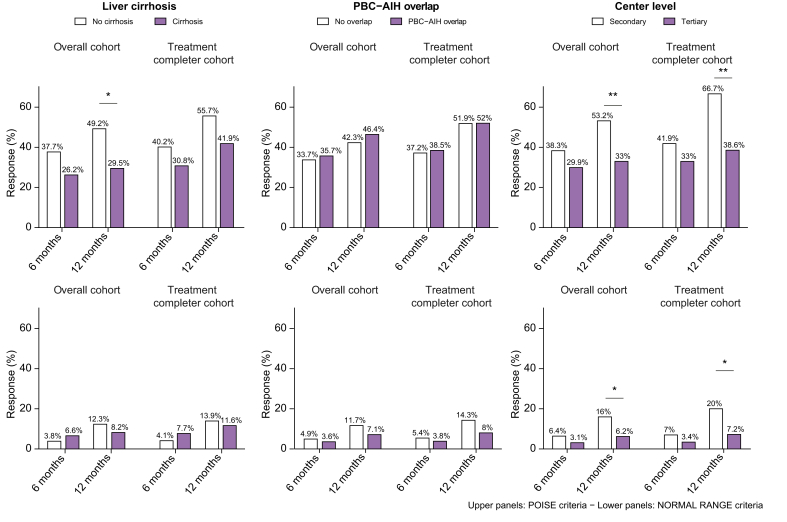
Patients were recruited into the Italian PBC Registry, a multicentre, observational cohort study that monitors patients with PBC at national level. The primary endpoint was the biochemical response according to ; the secondary endpoint was the biochemical response according to , defined as normal levels of bilirubin, alkaline phosphatase (ALP), and alanine aminotransferase (ALT) at 12 months. Safety and tolerability were also assessed.
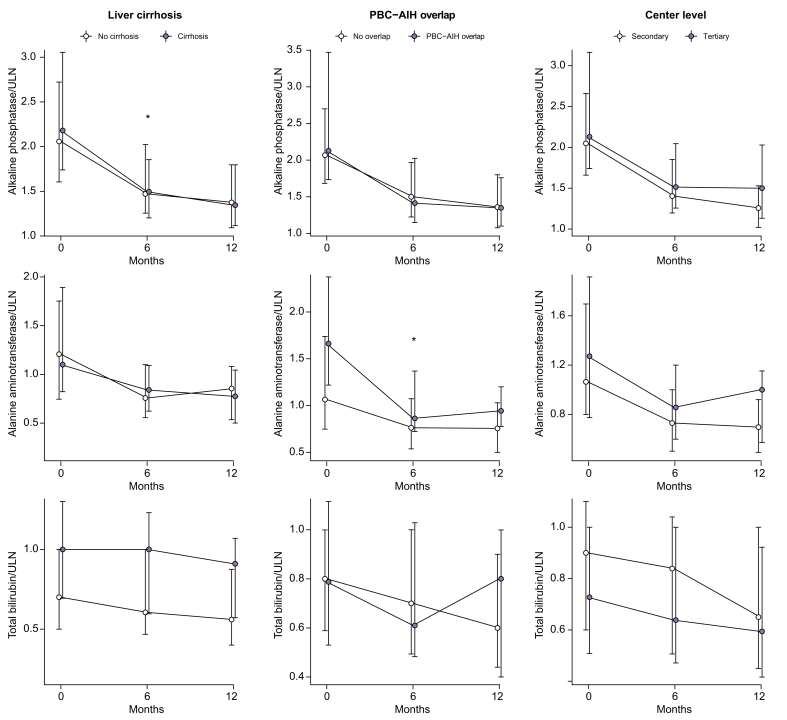
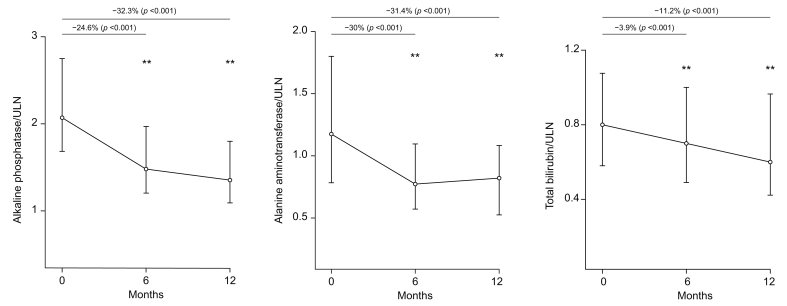
We analysed 191 patients until at least 12 months of follow-up. Median age was 57 years, 94% female, 61 (32%) had cirrhosis, 28 (15%) had histologically proven overlap with autoimmune hepatitis (PBC-AIH). At 12 months, significant median reductions of ALP (-32.3%), ALT (-31.4%), and bilirubin (-11.2%) were observed. Response rates were 42.9% according to , and 11% by . Patients with cirrhosis had lower response than patients without cirrhosis (29.5% 49.2%, = 0.01), owing to a higher rate of OCA discontinuation (30% 12%, = 0.004), although with similar ALP reduction (29.4% 34%, = 0.53). Overlap PBC-AIH had a similar response to pure PBC (46.4% 42.3%, = 0.68), with higher ALT reduction at 6 months (-38% -29%, = 0.04). Thirty-three patients (17%) prematurely discontinued OCA because of adverse events, of whom 11 experienced serious adverse events. Treatment-induced pruritus was the leading cause of OCA discontinuation (67%).
Effectiveness and safety of OCA under real-world conditions mirror those in the Poise trial. Patients with cirrhosis had lower tolerability. Overlap PBC-AIH showed higher ALT reduction at 6 months compared with patients with pure PBC.
Obeticholic acid (OCA) was shown to be effective in more than one-third of patients not responding to ursodeoxycholic acid in a real-world context in Italy. Patients with cirrhosis had more side effects with OCA, and this led to suspension of the drug in one-third of patients. OCA was also effective in patients who had overlap between autoimmune hepatitis and primary biliary cholangitis.
奥贝胆酸(OCA)是被批准用于原发性胆汁性胆管炎(PBC)患者且对熊去氧胆酸反应不足或不耐受的二线治疗药物。我们旨在评估OCA在实际临床环境中的有效性和安全性。
患者被纳入意大利PBC注册研究,这是一项多中心观察性队列研究,在全国范围内监测PBC患者。主要终点是根据[具体标准1]的生化反应;次要终点是根据[具体标准2]的生化反应,定义为12个月时胆红素、碱性磷酸酶(ALP)和丙氨酸氨基转移酶(ALT)水平正常。同时评估安全性和耐受性。
我们分析了191例患者,随访至少12个月。中位年龄为57岁,94%为女性,61例(32%)有肝硬化,28例(15%)经组织学证实与自身免疫性肝炎重叠(PBC-AIH)。12个月时,观察到ALP(-32.3%)、ALT(-31.4%)和胆红素(-11.2%)的中位数显著降低。根据[具体标准1]的缓解率为42.9%,根据[具体标准2]为11%。肝硬化患者的缓解率低于无肝硬化患者(29.5%对49.2%,P = 0.01),这是由于OCA停药率较高(30%对12%,P = 0.004),尽管ALP降低幅度相似(29.4%对34%,P = 0.53)。PBC-AIH重叠患者与单纯PBC患者的缓解情况相似(46.4%对42.3%,P = 0.68),6个月时ALT降低幅度更大(-38%对-29%,P = 0.04)。33例患者(17%)因不良事件提前停用OCA,其中11例经历了严重不良事件。治疗引起的瘙痒是OCA停药的主要原因(67%)。
OCA在实际临床环境中的有效性和安全性与Poise试验中的情况相似。肝硬化患者的耐受性较低。与单纯PBC患者相比,PBC-AIH重叠患者在6个月时ALT降低幅度更大。
在意大利的实际临床环境中,奥贝胆酸(OCA)在超过三分之一对熊去氧胆酸无反应的患者中显示出有效性。肝硬化患者使用OCA的副作用更多,这导致三分之一的患者停药。OCA在自身免疫性肝炎与原发性胆汁性胆管炎重叠的患者中也有效。