MD. Assistant Professor, Department of Emergency Medicine, Düzce University School of Medicine, Düzce, Turkey.
MD. Attending Emergency Physician, Department of Emergency Medicine, University of Health Sciences, Bakırköy Dr. Sadi Konuk Training and Research Hospital, Istanbul, Turkey.
Sao Paulo Med J. 2021 Mar-Apr;139(2):170-177. doi: 10.1590/1516-3180.2020.0649.R1.10122020.
Healthcare institutions are confronted with large numbers of patient admissions during large-scale or long-term public health emergencies like pandemics. Appropriate and effective triage is needed for effective resource use.
To evaluate the effectiveness of the Pandemic Medical Early Warning Score (PMEWS), Simple Triage Scoring System (STSS) and Confusion, Uremia, Respiratory rate, Blood pressure and age ≥ 65 years (CURB-65) score in an emergency department (ED) triage setting.
Retrospective study in the ED of a tertiary-care university hospital in Düzce, Turkey.
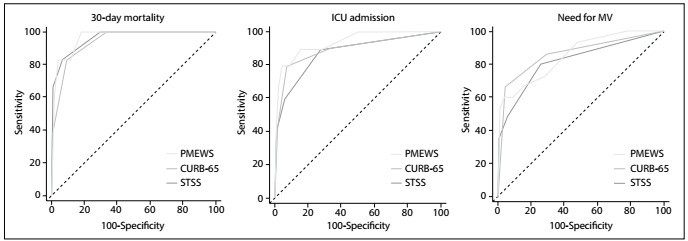
PMEWS, STSS and CURB-65 scores of patients diagnosed with COVID-19 pneumonia were calculated. Thirty-day mortality, intensive care unit (ICU) admission, mechanical ventilation (MV) need and outcomes were recorded. The predictive accuracy of the scores was assessed using receiver operating characteristic curve analysis.
One hundred patients with COVID-19 pneumonia were included. The 30-day mortality was 6%. PMEWS, STSS and CURB-65 showed high performance for predicting 30-day mortality (area under the curve: 0.968, 0.962 and 0.942, respectively). Age > 65 years, respiratory rate > 20/minute, oxygen saturation (SpO2) < 90% and ED length of stay > 4 hours showed associations with 30-day mortality (P < 0.05).
CURB-65, STSS and PMEWS scores are useful for predicting mortality, ICU admission and MV need among patients diagnosed with COVID-19 pneumonia. Advanced age, increased respiratory rate, low SpO2 and prolonged ED length of stay may increase mortality. Further studies are needed for developing the triage scoring systems, to ensure effective long-term use of healthcare service capacity during pandemics.
在大流行等大规模或长期公共卫生突发事件期间,医疗机构面临大量患者入院。需要进行适当有效的分诊,以有效利用资源。
评估 Pandemic Medical Early Warning Score (PMEWS)、Simple Triage Scoring System (STSS) 和 Confusion, Uremia, Respiratory rate, Blood pressure and age ≥ 65 years (CURB-65) 评分在急诊科分诊中的有效性。
在土耳其 Düzce 的一家三级保健大学医院的急诊科进行回顾性研究。
计算诊断为 COVID-19 肺炎的患者的 PMEWS、STSS 和 CURB-65 评分。记录 30 天死亡率、重症监护病房(ICU)入院、机械通气(MV)需求和结果。使用受试者工作特征曲线分析评估评分的预测准确性。
共纳入 100 例 COVID-19 肺炎患者。30 天死亡率为 6%。PMEWS、STSS 和 CURB-65 对预测 30 天死亡率具有较高的性能(曲线下面积分别为 0.968、0.962 和 0.942)。年龄 > 65 岁、呼吸频率 > 20/min、氧饱和度(SpO2)< 90%和急诊科停留时间 > 4 小时与 30 天死亡率相关(P < 0.05)。
CURB-65、STSS 和 PMEWS 评分可用于预测 COVID-19 肺炎患者的死亡率、ICU 入院和 MV 需求。高龄、呼吸频率增加、低 SpO2 和急诊科停留时间延长可能会增加死亡率。需要进一步研究以开发分诊评分系统,以确保在大流行期间有效利用医疗服务能力。