Faculty of Medicine and Health Sciences, Ghent University Hospital, Ghent, Belgium.
Department of Intensive Care Medicine, Ghent University Hospital, Ghent, Belgium.
Eur Geriatr Med. 2021 Aug;12(4):695-723. doi: 10.1007/s41999-021-00454-y. Epub 2021 Mar 8.
We aimed to collect the available evidence on outcome regarding survival and quality of life after cardiopulmonary resuscitation (CPR) following both in-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA) in the older population.
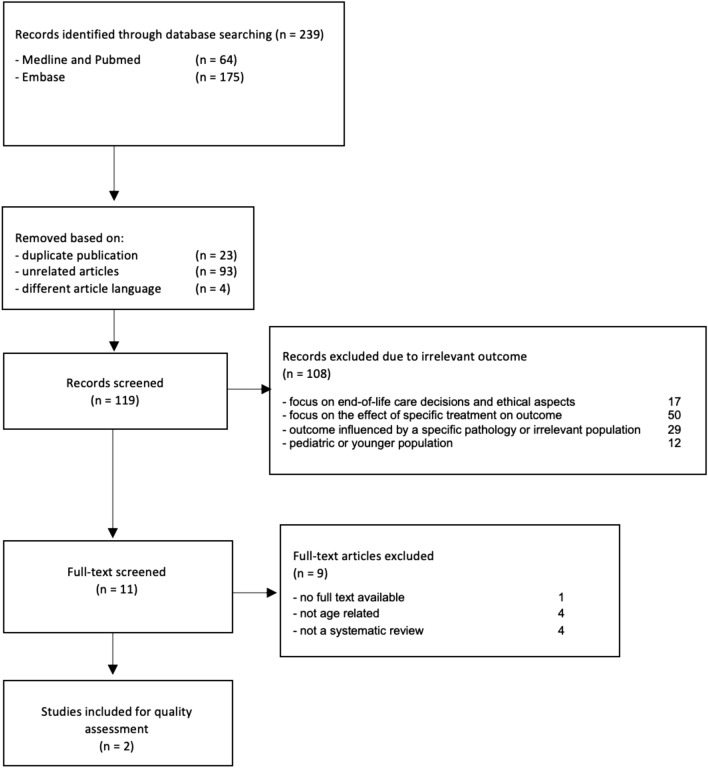
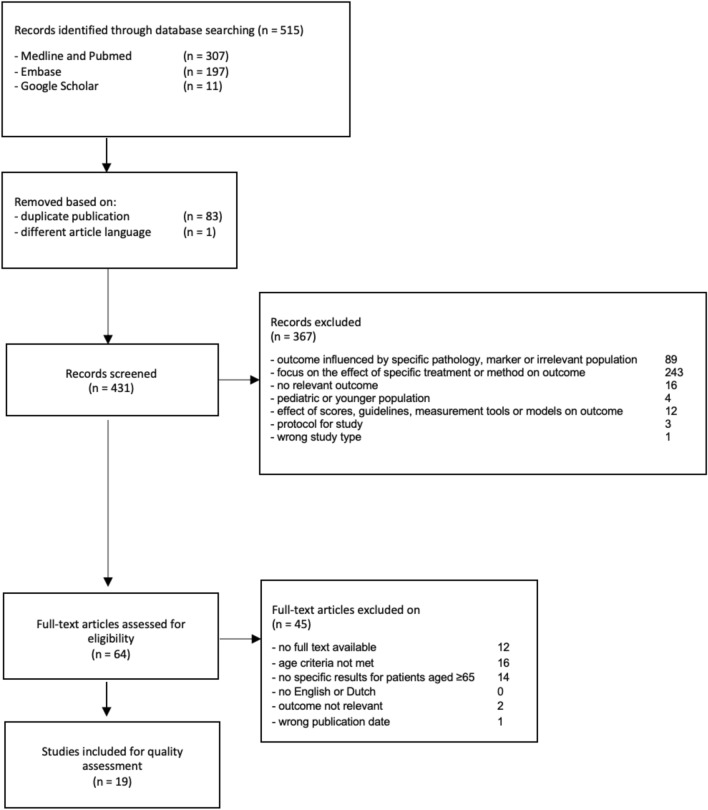
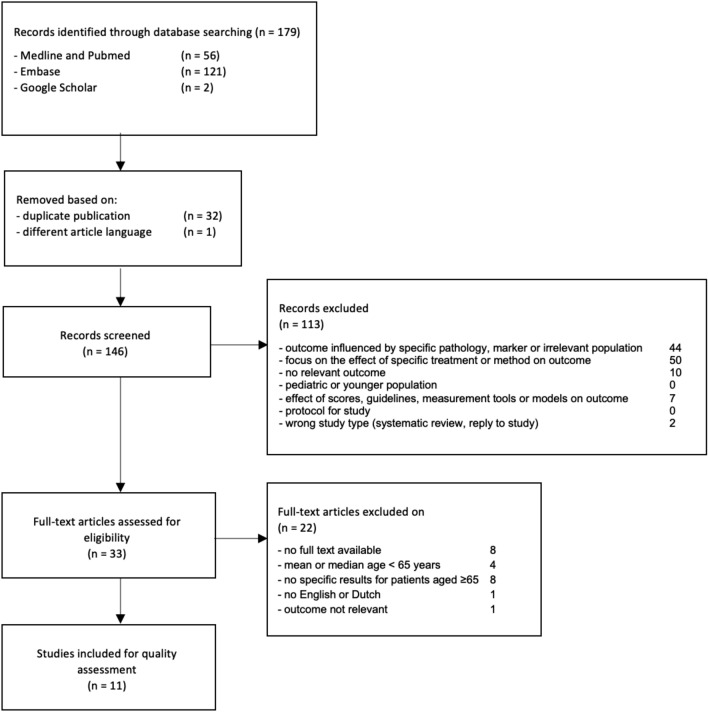
A scoping review was performed studying published reviews after 2008, focusing on outcome of CPR in patients aged ≥ 70 years following IHCA and OHCA. In addition, 11 (IHCA) and 19 (OHCA) eligible studies published after the 2 included reviews were analyzed regarding: return of spontaneous circulation, survival until hospital discharge, long-term survival, neurological outcome, discharge location or other measurements for quality of life (QoL).
The survival until hospital discharge ranged between 11.6 and 28.5% for IHCA and 0-11.1% for OHCA, and declined with increasing age. The same trend was seen regarding 1-year survival rates with 5.7-25.0% and 0-10% following IHCA and OHCA, respectively. A good neurological outcome defined as a Cerebral Performance Category (CPC) 1-2 was found in 11.5-23.6% (IHCA) and up to 10.5% (OHCA) of all patients. However, the proportion of CPC 1-2 among patients surviving until hospital discharge was 82-93% (IHCA) and 77-91.6% (OHCA). Few studies included other QoL measures as an outcome variable. Other risk factors aside from age were identified, including nursing home residency, comorbidity, non-shockable rhythm, non-witnessed arrest. The level of frailty was not studied as a predictor of arrest outcome in the included studies.
Hospital survival rates following IHCA and OHCA in the older population improved in the recent decade, though do not exceed 28.5% and 11.1%, respectively. The effect of age on outcome remains controversial and age should not be used as the sole decision criterium whether to initiate CPR. Future research should study frailty and resilience as an independent predictor regardless of age, and add broader, extensive QoL measures as outcome variables.
本研究旨在收集有关在院内心搏骤停(IHCA)和院外心搏骤停(OHCA)后,对老年患者心肺复苏(CPR)的生存和生活质量结局的现有证据。
本研究进行了范围综述,研究了 2008 年后发表的综述,重点关注≥70 岁的 IHCA 和 OHCA 患者的 CPR 结局。此外,还分析了纳入的 2 篇综述后发表的 11 项(IHCA)和 19 项(OHCA)符合条件的研究,内容包括自主循环恢复、出院时生存率、长期生存率、神经功能结局、出院地点或其他生活质量(QoL)测量。
IHCA 出院时生存率为 11.6%至 28.5%,OHCA 为 0%至 11.1%,且随年龄增长而下降。1 年生存率也呈现出同样的趋势,IHCA 和 OHCA 分别为 5.7%至 25.0%和 0%至 10%。所有患者中,定义为脑功能分类(CPC)1-2 的良好神经功能结局为 11.5%至 23.6%(IHCA)和高达 10.5%(OHCA)。然而,在出院时存活的患者中,CPC 1-2 的比例为 82%至 93%(IHCA)和 77%至 91.6%(OHCA)。少数研究将其他 QoL 测量作为结局变量。除年龄外,还确定了其他危险因素,包括疗养院居住、合并症、非可除颤节律、无目击者骤停。纳入的研究中未研究脆弱程度作为骤停结局的预测因素。
近十年来,老年人群 IHCA 和 OHCA 后院内生存率有所提高,但分别不超过 28.5%和 11.1%。年龄对结局的影响仍存在争议,年龄不应作为是否启动 CPR 的唯一决策标准。未来的研究应研究脆弱性和弹性作为独立的预测因素,而不论年龄如何,并增加更广泛、更全面的 QoL 测量作为结局变量。