Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, The Netherlands.
Netherlands Institute for Health Services Research (NIVEL), Utrecht, The Netherlands.
BMC Med. 2021 Mar 11;19(1):57. doi: 10.1186/s12916-021-01933-6.
Cardiometabolic diseases (CMD) are the major cause of death worldwide and are associated with a lower quality of life and high healthcare costs. To prevent a further rise in CMD and related healthcare costs, early detection and adequate management of individuals at risk could be an effective preventive strategy. The objective of this study was to determine long-term cost-effectiveness of stepwise CMD risk assessment followed by individualized treatment if indicated compared to care as usual. A computer-based simulation model was used to project long-term health benefits and cost-effectiveness, assuming the prevention program was implemented in Dutch primary care.
A randomized controlled trial in a primary care setting in which 1934 participants aged 45-70 years without recorded CMD or CMD risk factors participated. The intervention group was invited for stepwise CMD risk assessment through a risk score (step 1), additional risk assessment at the practice in case of increased risk (step 2) and individualized follow-up treatment if indicated (step 3). The control group was not invited for risk assessment, but completed a health questionnaire. Results of the effectiveness analysis on systolic blood pressure (- 2.26 mmHg; 95% CI - 4.01: - 0.51) and total cholesterol (- 0.15 mmol/l; 95% CI - 0.23: - 0.07) were used in this analysis. Outcome measures were the costs and benefits after 1-year follow-up and long-term (60 years) cost-effectiveness of stepwise CMD risk assessment compared to no assessment. A computer-based simulation model was used that included data on disability weights associated with age and disease outcomes related to CMD. Analyses were performed taking a healthcare perspective.
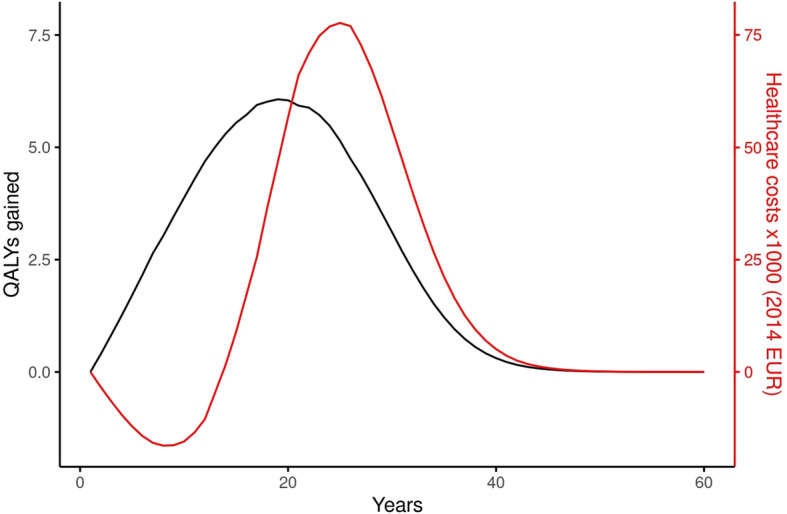
After 1 year, the average costs in the intervention group were 260 Euro higher than in the control group and differences were mainly driven by healthcare costs. No meaningful change was found in EQ 5D-based quality of life between the intervention and control groups after 1-year follow-up (- 0.0154; 95% CI - 0.029: 0.004). After 60 years, cumulative costs of the intervention were 41.4 million Euro and 135 quality-adjusted life years (QALY) were gained. Despite improvements in blood pressure and cholesterol, the intervention was not cost-effective (ICER of 306,000 Euro/QALY after 60 years). Scenario analyses did not allow for a change in conclusions with regard to cost-effectiveness of the intervention.
Implementation of this primary care-based CMD prevention program is not cost-effective in the long term. Implementation of this program in primary care cannot be recommended.
Dutch Trial Register NTR4277 , registered on 26 November 2013.
心血管代谢疾病(CMD)是全球主要的死亡原因,与生活质量下降和医疗保健成本高有关。为了防止 CMD 和相关医疗保健成本的进一步上升,对有风险的个体进行早期检测和适当管理可能是一种有效的预防策略。本研究的目的是确定逐步 CMD 风险评估的长期成本效益,如果需要,对指示进行个体化治疗,与常规护理相比。使用基于计算机的模拟模型来预测长期健康获益和成本效益,假设预防计划在荷兰初级保健中实施。
在初级保健环境中进行了一项随机对照试验,共有 1934 名年龄在 45-70 岁之间、无记录的 CMD 或 CMD 风险因素的参与者参加。干预组通过风险评分(第 1 步)邀请进行逐步 CMD 风险评估,如果风险增加,则在实践中进行额外的风险评估(第 2 步),如果需要,则进行个体化随访治疗(第 3 步)。对照组没有被邀请进行风险评估,但完成了健康问卷。本分析使用了有效性分析中收缩压(-2.26mmHg;95%CI-4.01:-0.51)和总胆固醇(-0.15mmol/l;95%CI-0.23:-0.07)的结果。本分析比较了逐步 CMD 风险评估与不评估的 1 年随访和长期(60 年)成本效益。使用了基于计算机的模拟模型,其中包括与年龄相关的残疾权重数据和与 CMD 相关的疾病结果。分析从医疗保健角度进行。
干预组的平均成本在第 1 年比对照组高 260 欧元,差异主要由医疗保健成本驱动。干预组和对照组在 1 年随访后的 EQ 5D 基于质量的生活没有明显变化(-0.0154;95%CI-0.029:0.004)。60 年后,干预组累计成本为 4140 万欧元,获得 135 个质量调整生命年(QALY)。尽管血压和胆固醇有所改善,但该干预措施并不具有成本效益(60 年后的 ICER 为 306,000 欧元/QALY)。情景分析并不能改变干预措施的成本效益结论。
该基于初级保健的 CMD 预防计划的实施在长期内不具有成本效益。不能推荐在初级保健中实施该计划。
荷兰试验注册 NTR4277,于 2013 年 11 月 26 日注册。