Division of Cardiology, Department of Internal Medicine, Chi-Mei Medical Center, Tainan, Taiwan.
Department of Public Health, College of Medicine, National Cheng Kung University, No. 1, University Road, Tainan, 701, Taiwan.
Sci Rep. 2021 Mar 10;11(1):5608. doi: 10.1038/s41598-021-84853-y.
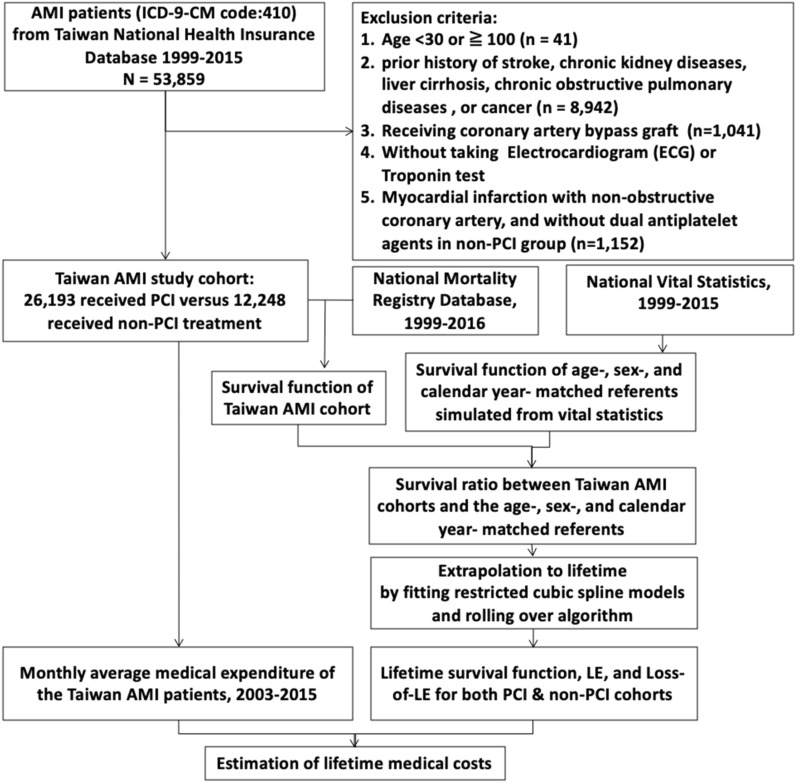
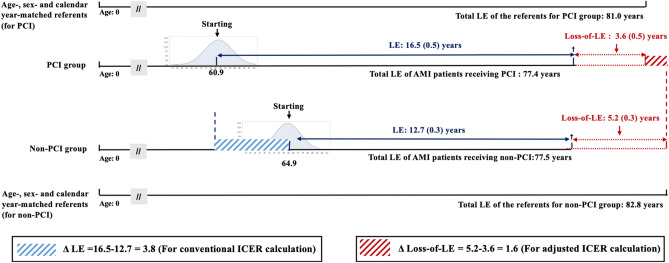
Although some studies have assessed the cost-effectiveness of percutaneous coronary intervention (PCI) in acute myocardial infarction (AMI), there has been a lack of nationwide real-world studies estimating life expectancy (LE), loss-of-LE, life-years saved, and lifetime medical costs. We evaluated the cost-effectiveness of PCI versus non-PCI therapy by integrating a survival function and mean-cost function over a lifelong horizon to obtain the estimations for AMI patients without major comorbidities. We constructed a longitudinal AMI cohort based on the claim database of Taiwan's National Health Insurance during 1999-2015. Taiwan's National Mortality Registry Database was linked to derive a survival function to estimate LE, loss-of-LE, life-years saved, and lifetime medical costs in both therapies. This study enrolled a total of 38,441 AMI patients; AMI patients receiving PCI showed a fewer loss-of-LE (3.6 versus 5.2 years), and more lifetime medical costs (US$ 49,112 versus US$ 43,532). The incremental cost-effectiveness ratio (ICER) was US$ 3488 per life-year saved. After stratification by age, the AMI patients aged 50-59 years receiving PCI was shown to be cost-saving. From the perspective of Taiwan's National Health Insurance, PCI is cost-effective in AMI patients without major comorbidities. Notably, for patients aged 50-59 years, PCI is cost-saving.
尽管已有一些研究评估了经皮冠状动脉介入治疗(PCI)在急性心肌梗死(AMI)中的成本效益,但缺乏全国范围内真实世界研究来评估预期寿命(LE)、LE 损失、节省的生命年数和终生医疗成本。我们通过整合生存函数和终生平均成本函数来评估 PCI 与非 PCI 治疗的成本效益,以获得无重大合并症的 AMI 患者的估计值。我们基于台湾全民健康保险 1999-2015 年的理赔数据库构建了一个纵向 AMI 队列。通过链接台湾国家死亡率登记数据库来获得生存函数,以估计两种治疗方法的 LE、LE 损失、节省的生命年数和终生医疗成本。本研究共纳入 38441 名 AMI 患者;接受 PCI 的 AMI 患者 LE 损失较少(3.6 年比 5.2 年),终生医疗成本较高(49112 美元比 43532 美元)。增量成本效益比(ICER)为每挽救 1 个生命年 3488 美元。按年龄分层后,接受 PCI 的 50-59 岁 AMI 患者显示为成本节约。从台湾全民健康保险的角度来看,无重大合并症的 AMI 患者接受 PCI 具有成本效益。值得注意的是,对于 50-59 岁的患者,PCI 是成本节约的。