Clinical Research Department, London School of Hygiene and Tropical Medicine, Keppel Street, London, United Kingdom.
Infectious Diseases Institute, Makerere University, Kampala, Uganda.
Clin Infect Dis. 2021 Sep 7;73(5):876-884. doi: 10.1093/cid/ciab162.
High-dose rifampicin may improve outcomes of tuberculous meningitis (TBM). Little safety or pharmacokinetic (PK) data exist on high-dose rifampicin in human immunodeficiency virus (HIV) coinfection, and no cerebrospinal fluid (CSF) PK data exist from Africa. We hypothesized that high-dose rifampicin would increase serum and CSF concentrations without excess toxicity.
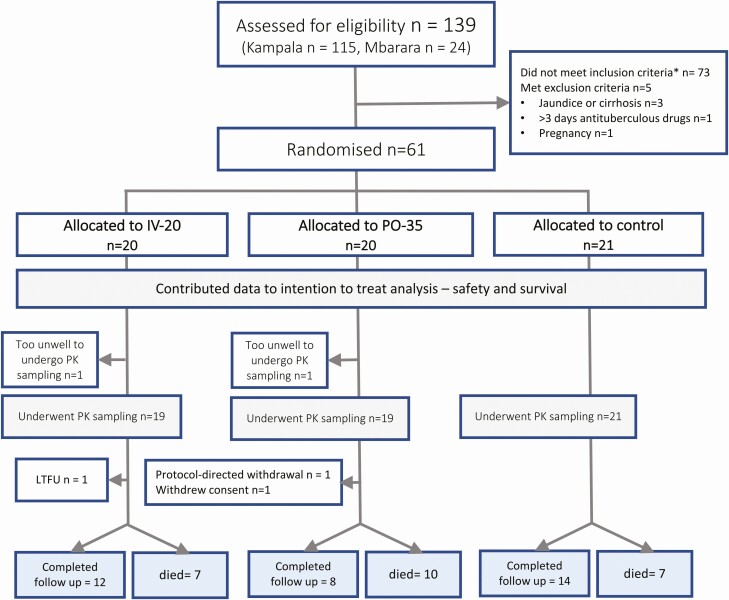
In this phase II open-label trial, Ugandan adults with suspected TBM were randomized to standard-of-care control (PO-10, rifampicin 10 mg/kg/day), intravenous rifampicin (IV-20, 20 mg/kg/day), or high-dose oral rifampicin (PO-35, 35 mg/kg/day). We performed PK sampling on days 2 and 14. The primary outcomes were total exposure (AUC0-24), maximum concentration (Cmax), CSF concentration, and grade 3-5 adverse events.
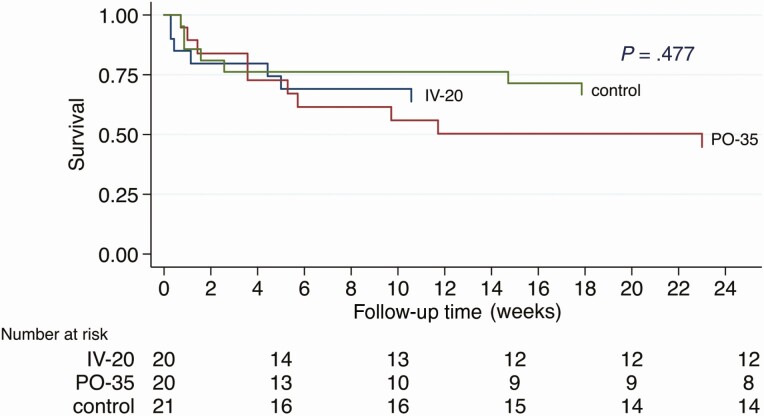
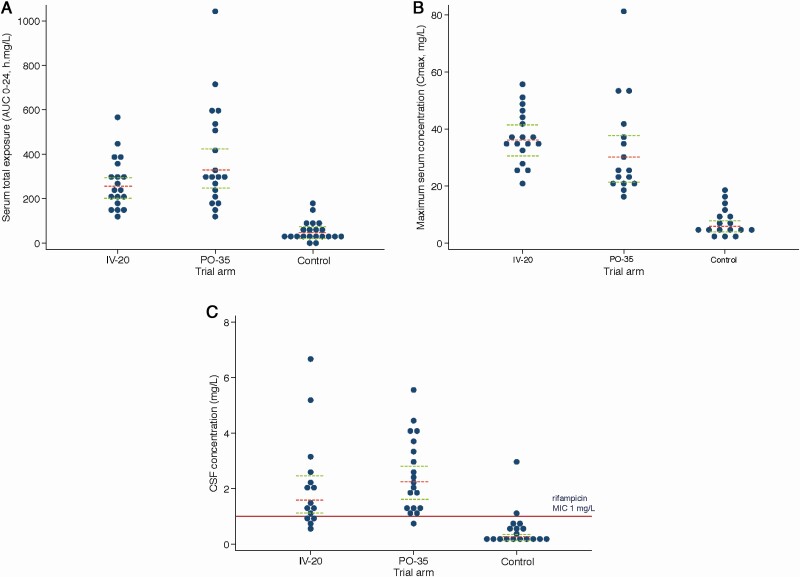
We enrolled 61 adults, 92% were living with HIV, median CD4 count was 50 cells/µL (interquartile range [IQR] 46-56). On day 2, geometric mean plasma AUC0-24hr was 42.9·h mg/L with standard-of-care 10 mg/kg dosing, 249·h mg/L for IV-20 and 327·h mg/L for PO-35 (P < .001). In CSF, standard of care achieved undetectable rifampicin concentration in 56% of participants and geometric mean AUC0-24hr 0.27 mg/L, compared with 1.74 mg/L (95% confidence interval [CI] 1.2-2.5) for IV-20 and 2.17 mg/L (1.6-2.9) for PO-35 regimens (P < .001). Achieving CSF concentrations above rifampicin minimal inhibitory concentration (MIC) occurred in 11% (2/18) of standard-of-care, 93% (14/15) of IV-20, and 95% (18/19) of PO-35 participants. Higher serum and CSF levels were sustained at day 14. Adverse events did not differ by dose (P = .34).
Current international guidelines result in sub-therapeutic CSF rifampicin concentration for 89% of Ugandan TBM patients. High-dose intravenous and oral rifampicin were safe and respectively resulted in exposures ~6- and ~8-fold higher than standard of care, and CSF levels above the MIC.
高剂量利福平可能改善结核性脑膜炎(TBM)的预后。人免疫缺陷病毒(HIV)合并感染患者应用高剂量利福平的安全性和药代动力学(PK)数据较少,来自非洲的脑脊液(CSF)PK 数据也很少。我们假设高剂量利福平可增加血清和 CSF 浓度,而不会增加毒性。
在这项 II 期开放标签试验中,乌干达疑似 TBM 的成年人被随机分配至标准治疗对照(PO-10,利福平 10 mg/kg/天)、静脉利福平(IV-20,20 mg/kg/天)或高剂量口服利福平(PO-35,35 mg/kg/天)。我们在第 2 天和第 14 天进行 PK 采样。主要结局是总暴露(AUC0-24)、最大浓度(Cmax)、CSF 浓度和 3-5 级不良事件。
我们共纳入 61 名成年人,92%合并 HIV 感染,中位 CD4 计数为 50 个细胞/µL(四分位间距 [IQR] 46-56)。第 2 天时,标准治疗 10 mg/kg 剂量组的血浆 AUC0-24hr 几何均数为 42.9·h mg/L,IV-20 组为 249·h mg/L,PO-35 组为 327·h mg/L(P<.001)。CSF 中,标准治疗组 56%的参与者检测不到利福平浓度,AUC0-24hr 几何均数为 0.27 mg/L,而 IV-20 组为 1.74 mg/L(95%置信区间 [CI] 1.2-2.5),PO-35 组为 2.17 mg/L(1.6-2.9)(P<.001)。标准治疗组、IV-20 组和 PO-35 组 CSF 浓度达到利福平最低抑菌浓度(MIC)以上的比例分别为 11%(2/18)、93%(14/15)和 95%(18/19)。第 14 天时,血清和 CSF 水平仍保持较高水平。不同剂量组的不良事件发生率无差异(P=.34)。
目前的国际指南导致 89%的乌干达 TBM 患者 CSF 中的利福平浓度低于治疗范围。高剂量静脉和口服利福平分别使暴露量比标准治疗组增加 6 倍和 8 倍,CSF 浓度高于 MIC。