Wellcome Centre for Infectious Diseases Research in Africa, Institute for Infectious Disease and Molecular Medicine, University of Cape Town, Cape Town, South Africa.
Division of Infectious Diseases and HIV Medicine, Department of Medicine, University of Cape Town, Cape Town, South Africa.
Antimicrob Agents Chemother. 2021 Jul 16;65(8):e0014021. doi: 10.1128/AAC.00140-21.
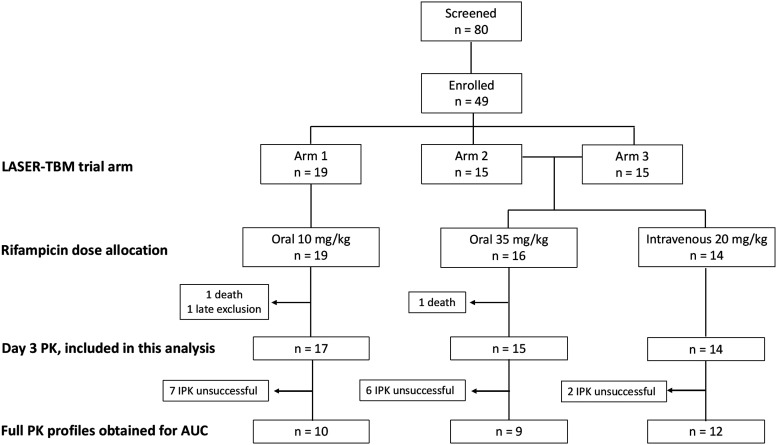
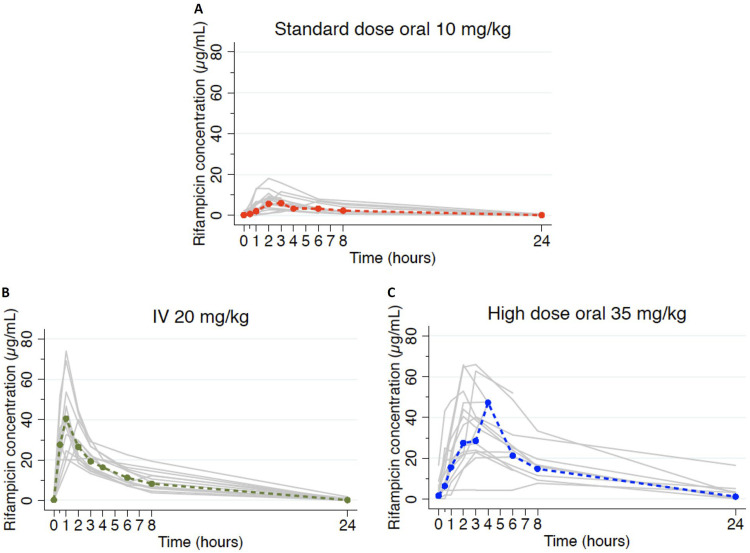
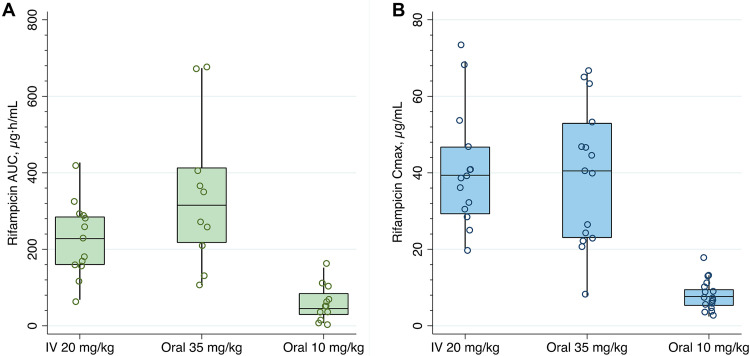
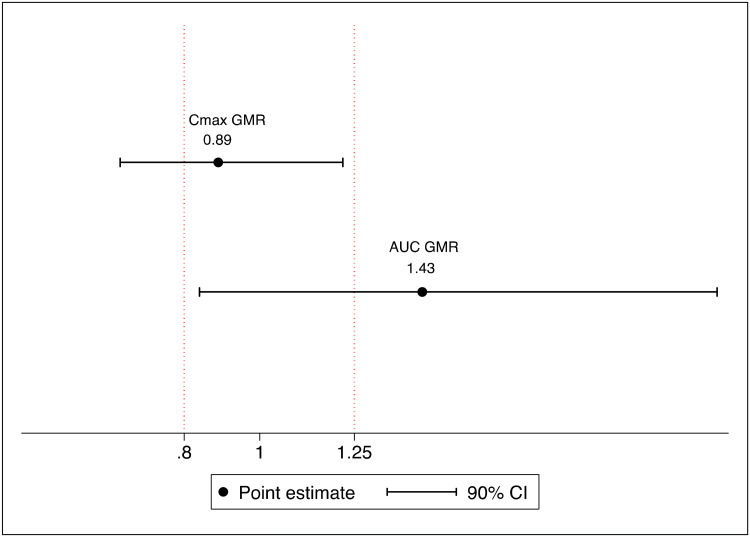
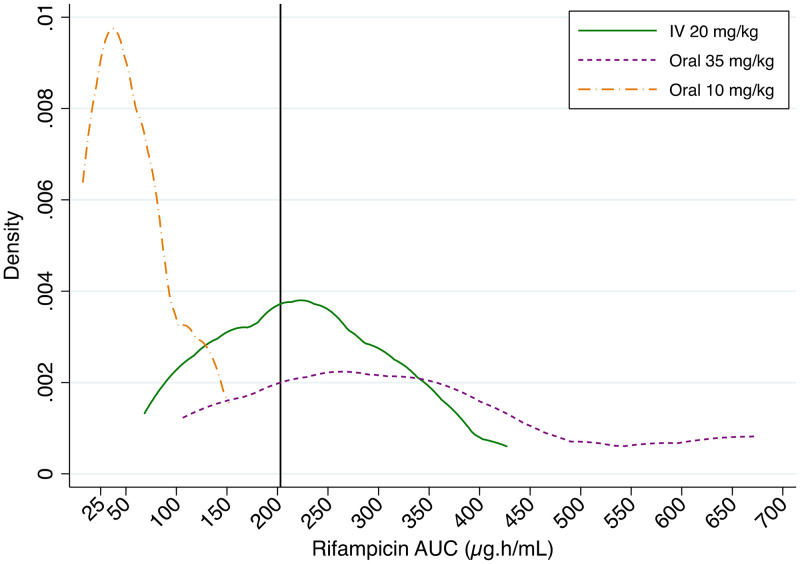
Higher doses of intravenous rifampicin may improve outcomes in tuberculous meningitis but are impractical in high-burden settings. We hypothesized that plasma rifampicin exposures would be similar between oral dosing of 35 mg/kg of body weight and intravenous dosing of 20 mg/kg, which has been proposed for efficacy trials in tuberculous meningitis. We performed a randomized parallel-group pharmacokinetic study nested within a clinical trial of intensified antimicrobial therapy for tuberculous meningitis. HIV-positive participants with tuberculous meningitis were recruited from South African hospitals and randomized to one of three rifampicin dosing groups: standard (oral 10 mg/kg), high dose (oral 35 mg/kg), and intravenous (20 mg/kg). Intensive pharmacokinetic sampling was done on day 3. Data were described using noncompartmental analysis, and exposures were compared by geometric mean ratios (GMRs). Forty-six participants underwent pharmacokinetic sampling (standard dose, = 17; high-dose oral, = 15; intravenous, = 14). The median CD4 count was 130 cells/mm (interquartile range [IQR], 66 to 253 cells/mm). The rifampicin geometric mean area under the concentration-time curve from 0 to 24 h (AUC) values were 42.9 μg · h/ml (95% confidence interval [CI], 24.5 to 75.0 μg · h/ml) for the standard dose, 295.2 μg · h/ml (95% CI, 189.9 to 458.8 μg · h/ml) for the high oral dose, and 206.5 μg · h/ml (95% CI, 154.6 to 275.8 μg · h/ml) for intravenous administration. The rifampicin AUC GMR was 1.44 (90% CI, 0.84 to 2.21) and the maximal concentration of drug in serum () GMR was 0.89 (90% CI, 0.63 to 1.23) for high-dose oral administration with respect to intravenous dosing. The plasma rifampicin AUC was higher after an oral 35-mg/kg dose than with intravenous administration at a 20-mg/kg dose over the first few days of tuberculosis (TB) treatment. The findings support oral rifampicin dosing in future tuberculous meningitis trials.
高剂量静脉利福平可能改善结核性脑膜炎的结局,但在高负担环境下不切实际。我们假设,口服 35mg/kg 体重与静脉注射 20mg/kg 体重的利福平暴露量相似,这已被提议用于结核性脑膜炎的疗效试验。我们进行了一项随机平行组药代动力学研究,该研究嵌套在结核性脑膜炎强化抗菌治疗的临床试验中。从南非医院招募了 HIV 阳性结核性脑膜炎患者,并随机分为三组利福平剂量组:标准剂量(口服 10mg/kg)、高剂量(口服 35mg/kg)和静脉注射(20mg/kg)。在第 3 天进行了强化药代动力学采样。使用非房室分析描述数据,并通过几何均数比值(GMR)比较暴露量。46 名参与者接受了药代动力学采样(标准剂量组, = 17;高剂量口服组, = 15;静脉注射组, = 14)。中位 CD4 计数为 130 个细胞/mm(四分位间距[IQR],66 至 253 个细胞/mm)。标准剂量组的利福平 0 至 24 小时浓度-时间曲线下面积(AUC)的几何平均值为 42.9μg·h/ml(95%置信区间[CI],24.5 至 75.0μg·h/ml),高口服剂量组为 295.2μg·h/ml(95%CI,189.9 至 458.8μg·h/ml),静脉注射组为 206.5μg·h/ml(95%CI,154.6 至 275.8μg·h/ml)。高剂量口服组的利福平 AUC GMR 为 1.44(90%CI,0.84 至 2.21),最大血清药物浓度( )GMR 为 0.89(90%CI,0.63 至 1.23),与静脉注射组相比。在结核病(TB)治疗的最初几天,口服 35mg/kg 剂量后的利福平 AUC 高于静脉注射 20mg/kg 剂量。这些发现支持在未来的结核性脑膜炎试验中口服利福平给药。