Xin Wenqiang, Yang Shixue, Li Qifeng, Yang Xinyu
Department of Neurosurgery, Tianjin Medical University General Hospital, Tianjin, China.
Ann Transl Med. 2021 Feb;9(3):256. doi: 10.21037/atm-20-4620.
The incidence of stroke or death in carotid endarterectomy (CEA) versus carotid artery stenting (CAS) cannot be estimated accurately. We aimed to compare periprocedural stroke or death in patients with symptomatic or asymptomatic carotid artery stenosis (CS) treated with CEA versus CAS.
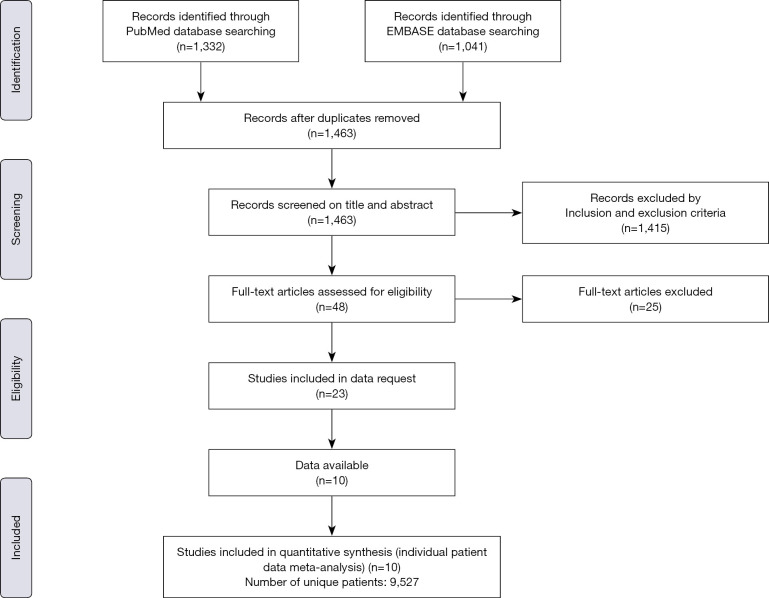
Ten randomized trials (with ≥100 randomized patients per trial) compared the relative effectiveness of CAS and CEA for the prevention of stroke or death.
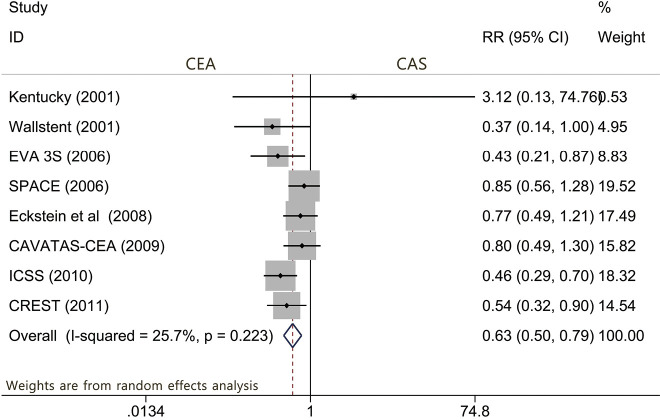
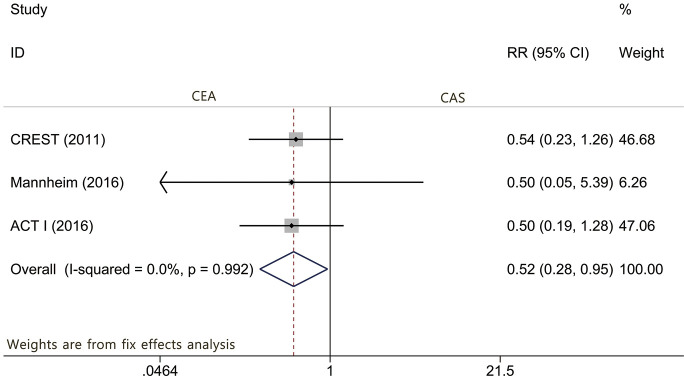
In the symptomatic group during the periprocedural period, the results showed that the risk of death or any stroke [risk ratio (RR): 0.627; 95% CI: 0.497-0.792; P<0.001] and the risk of any stroke (RR: 0.654; 95% CI: 0.522-0.820; P<0.001) were significantly greater with CAS than with CEA. The difference in the risk of periprocedural stroke was mostly attributed to nondisabling stroke (RR: 0.407; 95% CI: 0.264-0.627; P<0.001), which was driven especially by ipsilateral ischemic stroke (RR: 0.649; 95% CI: 0.494-0.851; P=0.002) and bradycardia or hypotension (RR: 0.105; 95% CI: 0.051-0.217; P<0.001). However, we found that the CEA group had a higher rate of myocardial infarction than the CAS group (RR: 2.496; P=0.025). Meanwhile, ipsilateral stenosis >70% increased the incidence of periprocedural death or stroke for post-CEA patients (RR: 2.166, 95% CI: 1.112 to 4.220, P=0.023), but no risk factors were identified for post-CAS. Regarding the asymptomatic group, the results demonstrated that patients randomized to CEA had a significantly reduced risk of periprocedural stroke (RR: 0.518; 95% CI: 0.281-0.954; P=0.035), which seems to be driven by periprocedural minor stroke (RR: 0.482; 95% CI: 0.231-0.982; P=0.046).
Among patients with symptomatic CS, CEA was associated with reduced rates of periprocedural stroke and periprocedural nondisabling stroke. Among patients with asymptomatic CS, the rates of minor stroke and stroke in general were higher with stenting than with CEA. Based on the current data, CEA is more beneficial than CAS for 30-day stroke prevention.
无法准确估计颈动脉内膜切除术(CEA)与颈动脉支架置入术(CAS)导致中风或死亡的发生率。我们旨在比较接受CEA与CAS治疗的有症状或无症状颈动脉狭窄(CS)患者围手术期的中风或死亡情况。
十项随机试验(每项试验随机患者≥100例)比较了CAS和CEA预防中风或死亡的相对有效性。
在有症状组的围手术期,结果显示,CAS组的死亡或任何中风风险[风险比(RR):0.627;95%置信区间(CI):0.497 - 0.792;P<0.001]和任何中风风险(RR:0.654;95%CI:0.522 - 0.820;P<0.001)均显著高于CEA组。围手术期中风风险的差异主要归因于非致残性中风(RR:0.407;95%CI:0.264 - 0.627;P<0.001),这尤其由同侧缺血性中风(RR:0.649;95%CI:0.494 - 0.851;P = 0.002)和心动过缓或低血压(RR:0.105;95%CI:0.051 - 0.217;P<0.()01)所致。然而,我们发现CEA组心肌梗死发生率高于CAS组(RR:2.496;P = 0.025)。同时,同侧狭窄>70%增加了CEA术后患者围手术期死亡或中风的发生率(RR:2.166,95%CI:1.112至4.220,P = 0.023),但未发现CAS术后的风险因素。对于无症状组,结果表明随机接受CEA治疗的患者围手术期中风风险显著降低(RR:0.518;95%CI:0.281 - 0.954;P = 0.035),这似乎是由围手术期轻微中风所致(RR:0.482;95%CI:0.231 - 0.982;P = 0.046)。
在有症状的CS患者中,CEA与围手术期中风和围手术期非致残性中风发生率降低相关。在无症状的CS患者中,支架置入术导致的轻微中风和总体中风发生率高于CEA。基于目前的数据,在预防30天中风方面,CEA比CAS更有益。