Department of Hepatobiliary Surgery, Fujian Provincial Hospital, the Shengli Clinical Medical College of Fujian Medical University, Fuzhou, 350001, Fujian, China.
Department of Hepatic Surgery VI, The Eastern Hepatobiliary Surgery Hospital, Second Military Medical University, 225 Changhai Road, Shanghai, 200433, China.
BMC Cancer. 2021 Mar 12;21(1):272. doi: 10.1186/s12885-021-07956-9.
Bile duct invasion is a relatively rare event and is not well characterised in hepatocellular carcinoma (HCC). It remains very difficult to diagnose HCC with bile duct tumour thrombus (BDTT) before surgery. Increasing evidence has revealed that inflammation plays a critical role in tumorigenesis. This study aimed to develop nomograms based on systemic and hepatic inflammation markers to predict microscopic BDTT (micro-BDTT) before surgery in HCC.
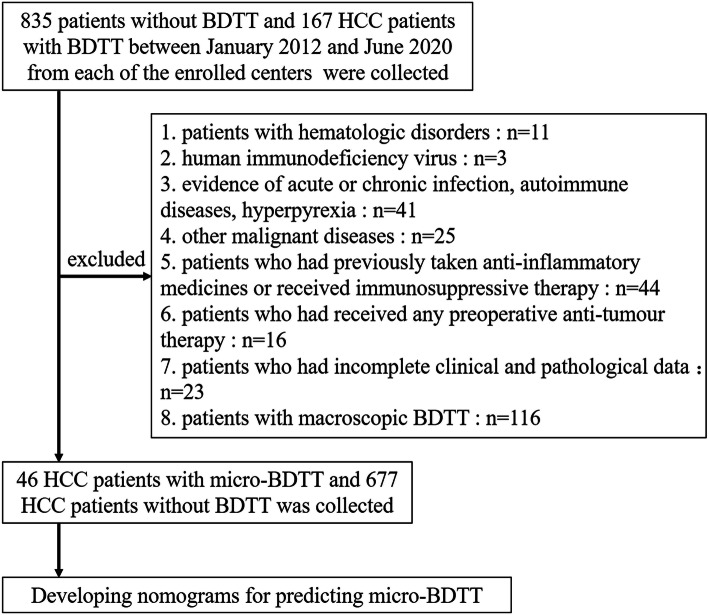
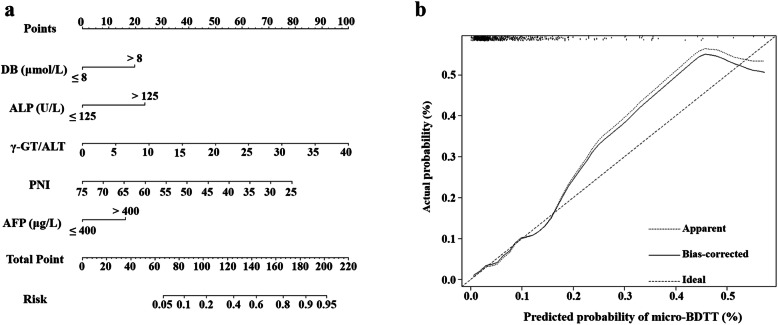
A total of 723 HCC patients who underwent hepatectomy as initial therapy between January 2012 and June 2020 were included in the study. Logistic regression analysis was used to identify independent risk factors for micro-BDTT. The nomograms were constructed using significant predictors, including α-fetoprotein (AFP), alkaline phosphatase (ALP), direct bilirubin (DB), prognostic nutritional index (PNI), and γ-glutamyl transferase (γ-GT)/alanine aminotransferase (ALT). The prediction accuracies of the nomograms were evaluated using the area under the receiver operating characteristic (ROC) curve.
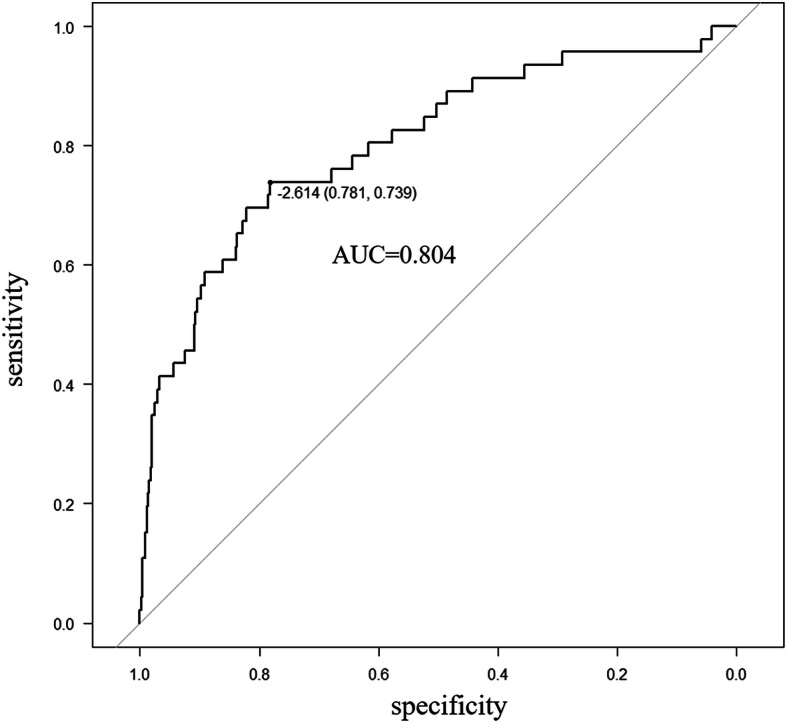
AFP, ALP, DB, PNI, and γ-GT/ALT were independent risk factors for predicting micro-BDTT (P = 0.036, P = 0.004, P = 0.013, P = 0.012, and P = 0.006, respectively), which were assembled into the nomograms. The area under the ROC curve of the nomograms combining PNI and γ-GT/ALT for predicting micro-BDTT was 0.804 (95% confidence interval [CI]: 0.730-0.878). The sensitivity and specificity values when used in predicting micro-BDTT before surgery were 0.739 (95% CI: 0.612-0.866) and 0.781 (95% CI: 0.750-0.813), respectively.
The nomogram based on combining systemic and hepatic inflammation markers is suitable for predicting micro-BDTT before surgery in HCC patients, leading to a rational therapeutic choice for HCC.
胆管侵犯在肝细胞癌(HCC)中较为罕见,特征也不明显。在手术前诊断 HCC 伴胆管癌栓(BDTT)仍然非常困难。越来越多的证据表明,炎症在肿瘤发生中起着关键作用。本研究旨在基于全身和肝脏炎症标志物建立预测 HCC 术前微小 BDTT(micro-BDTT)的列线图。
回顾性分析 2012 年 1 月至 2020 年 6 月期间接受肝切除术作为初始治疗的 723 例 HCC 患者。采用 logistic 回归分析确定 micro-BDTT 的独立危险因素。使用包括甲胎蛋白(AFP)、碱性磷酸酶(ALP)、直接胆红素(DB)、预后营养指数(PNI)和谷氨酰转肽酶/丙氨酸氨基转移酶(γ-GT/ALT)在内的显著预测因子构建列线图。通过受试者工作特征(ROC)曲线下面积评估列线图的预测准确性。
AFP、ALP、DB、PNI 和 γ-GT/ALT 是预测 micro-BDTT 的独立危险因素(P=0.036、P=0.004、P=0.013、P=0.012 和 P=0.006),这些因素被纳入列线图。结合 PNI 和 γ-GT/ALT 的列线图预测 micro-BDTT 的 ROC 曲线下面积为 0.804(95%置信区间[CI]:0.730-0.878)。用于预测 micro-BDTT 的列线图的术前灵敏度和特异性值分别为 0.739(95%CI:0.612-0.866)和 0.781(95%CI:0.750-0.813)。
基于全身和肝脏炎症标志物的列线图适用于预测 HCC 患者术前 micro-BDTT,有助于对 HCC 进行合理的治疗选择。