Department of Intensive Care, Amsterdam UMC, Vrije Universiteit Amsterdam, De Boelelaan 1117, mail stop ZH 7D-172, 1081HV, Amsterdam, The Netherlands.
Research VUmc Intensive Care (REVIVE), Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
Intensive Care Med. 2021 Apr;47(4):422-434. doi: 10.1007/s00134-021-06370-w. Epub 2021 Mar 13.
Most randomized controlled trials (RCTs) in patients with acute respiratory distress syndrome (ARDS) revealed indeterminate or conflicting study results. We aimed to systematically evaluate between-trial heterogeneity in reporting standards and trial outcome.
A systematic review of RCTs published between 2000 and 2019 was performed including adult ARDS patients receiving lung-protective ventilation. A random-effects meta-regression model was applied to quantify heterogeneity (non-random variability) and to evaluate trial and patient characteristics as sources of heterogeneity.
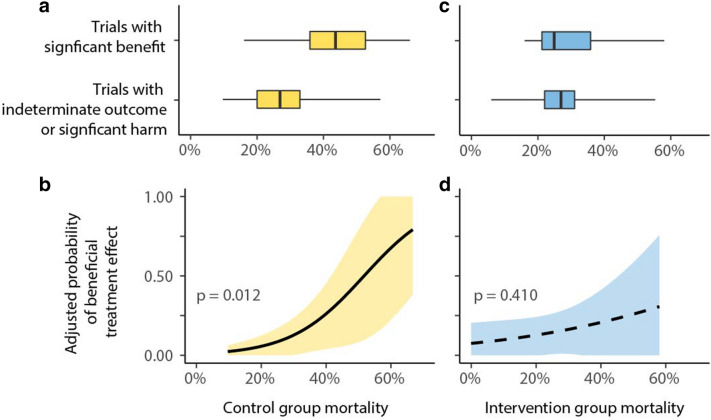
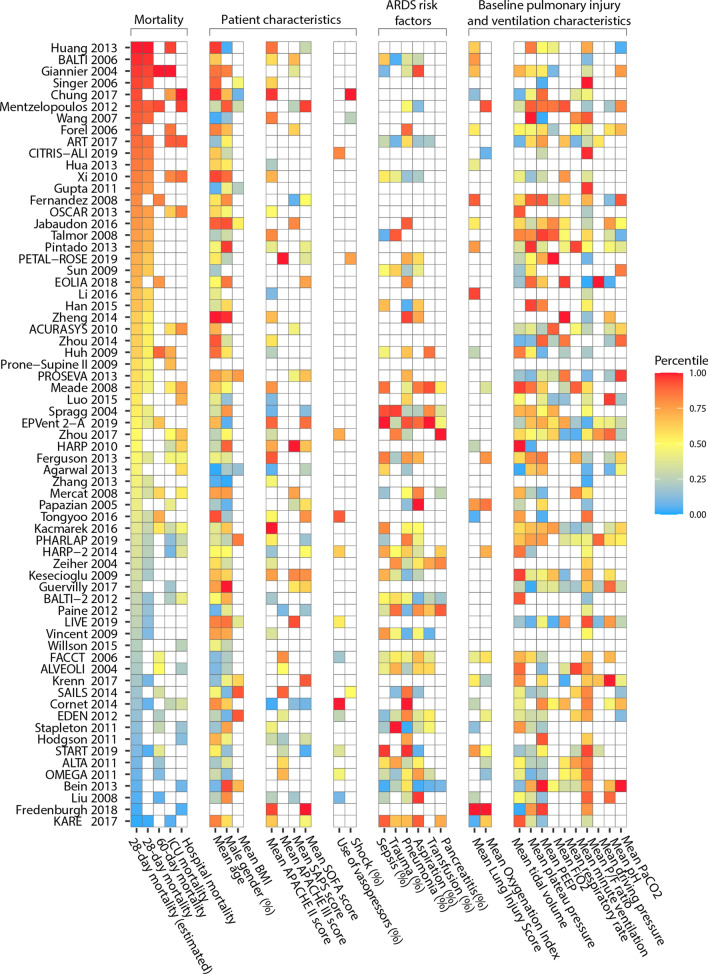
In total, 67 RCTs were included. The 28-day control-group mortality rate ranged from 10 to 67% with large non-random heterogeneity (I = 88%, p < 0.0001). Reported baseline patient characteristics explained some of the outcome heterogeneity, but only six trials (9%) reported all four independently predictive variables (mean age, mean lung injury score, mean plateau pressure and mean arterial pH). The 28-day control group mortality adjusted for patient characteristics (i.e. the residual heterogeneity) ranged from 18 to 45%. Trials with significant benefit in the primary outcome reported a higher control group mortality than trials with an indeterminate outcome or harm (mean 28-day control group mortality: 44% vs. 28%; p = 0.001).
Among ARDS RCTs in the lung-protective ventilation era, there was large variability in the description of baseline characteristics and significant unexplainable heterogeneity in 28-day control group mortality. These findings signify problems with the generalizability of ARDS research and underline the urgent need for standardized reporting of trial and baseline characteristics.
大多数急性呼吸窘迫综合征(ARDS)患者的随机对照试验(RCT)显示结果不确定或相互矛盾。我们旨在系统评估报告标准和试验结果之间的试验间异质性。
对 2000 年至 2019 年期间发表的成人 ARDS 患者接受肺保护性通气的 RCT 进行系统评价。应用随机效应荟萃回归模型量化异质性(非随机变异性),并评估试验和患者特征作为异质性的来源。
共纳入 67 项 RCT。对照组 28 天死亡率为 10%至 67%,存在较大的非随机异质性(I=88%,p<0.0001)。报告的基线患者特征解释了部分结局异质性,但只有 6 项试验(9%)报告了所有四个独立预测变量(平均年龄、平均肺损伤评分、平均平台压和平均动脉 pH)。调整患者特征后的 28 天对照组死亡率(即剩余异质性)为 18%至 45%。主要结局有显著获益的试验报告的对照组 28 天死亡率高于结局不确定或有害的试验(对照组 28 天死亡率:44% vs. 28%;p=0.001)。
在肺保护性通气时代的 ARDS RCT 中,基线特征的描述存在很大的变异性,28 天对照组死亡率存在显著的无法解释的异质性。这些发现表明 ARDS 研究的可推广性存在问题,并强调了标准化报告试验和基线特征的迫切需要。