Tarazan Nehal, Alshehri Moayad, Sharif Sameer, Al Duhailib Zainab, Møller Morten Hylander, Belley-Cote Emilie, Alshahrani Mohammed, Centofanti John, McIntyre Lauralyn, Baw Bandar, Meade Maureen, Alhazzani Waleed
Department of Medicine, McMaster University, Hamilton, Canada.
Department of Internal Medicine, King Saud University, Riyadh, Saudi Arabia.
Intensive Care Med Exp. 2020 Oct 23;8(1):61. doi: 10.1186/s40635-020-00348-6.
Existing clinical practice guidelines support the use of neuromuscular blocking agents (NMBA) in acute respiratory distress syndrome (ARDS); however, a recent large randomized clinical trial (RCT) has questioned this practice. Therefore, we updated a previous systematic review to determine the efficacy and safety of NMBAs in ARDS.
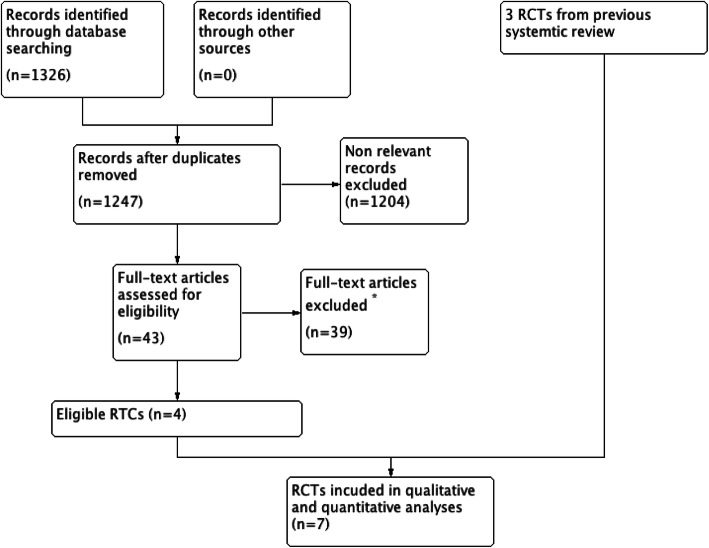
We searched MEDLINE, EMBASE (October 2012 to July 2019), the Cochrane (Central) database, and clinical trial registries ( ClinicalTrials.gov , ISRCTN Register, and WHO ICTRP) for RCTs comparing the effects of NMBA as a continuous infusion versus placebo or no NMBA infusion (but allowing intermittent NMBA boluses) on patient-important outcomes for adults with ARDS. Two independent reviewers assessed the methodologic quality of the primary studies and abstracted data.
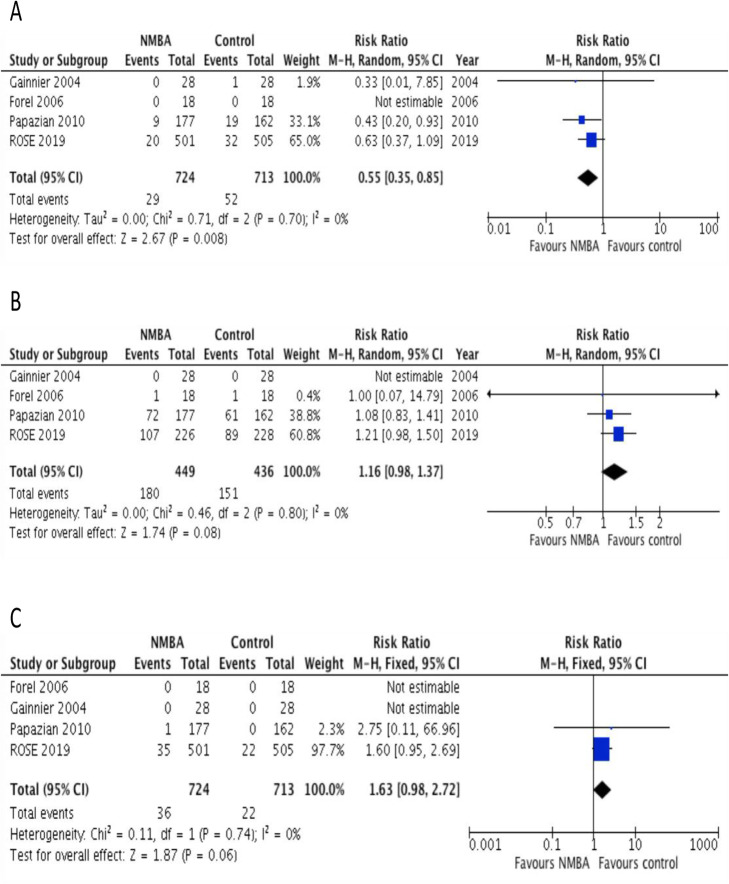
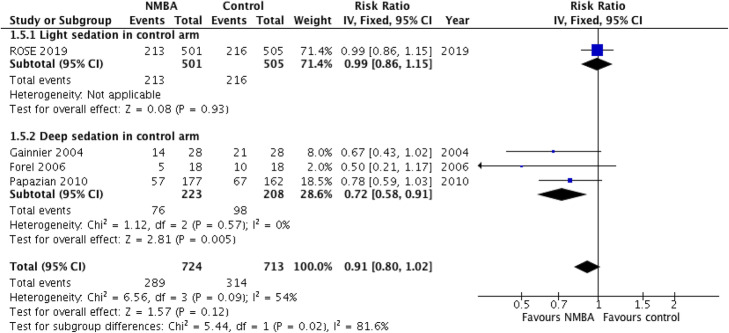
Seven RCTs, including four new RCTs, met eligibility criteria for this review. These trials enrolled 1598 patients with moderate to severe ARDS at centers in the USA, France, and China. All trials assessed short-term continuous infusions of cisatracurium or vecuronium. The pooled estimate for mortality outcomes showed significant statistical heterogeneity, which was only explained by a subgroup analysis by depth of sedation in the control arm. A continuous NMBA infusion did not improve mortality when compared to a light sedation strategy with no NMBA infusion (relative risk [RR] 0.99; 95% CI 0.86-1.15; moderate certainty; P = 0.93). On the other hand, continuous NMBA infusion reduced mortality when compared to deep sedation with as needed NMBA boluses (RR 0.71; 95% CI 0.57-0.89; low certainty; P = 0.003). Continuous NMBA infusion reduced the rate of barotrauma (RR 0.55; 95% CI 0.35-0.85, moderate certainty; P = 0.008) across eligible trials, but the effect on ventilator-free days, duration of mechanical ventilation, and ICU-acquired weakness was uncertain.
Inconsistency in study methods and findings precluded the pooling of all trials for mortality. In a pre-planned sensitivity analysis, the impact of NMBA infusion on mortality depends on the strategy used in the control arm, showing reduced mortality when compared to deep sedation, but no effect on mortality when compared to lighter sedation. In both situations, a continuous NMBA infusion may reduce the risk of barotrauma, but the effects on other patient-important outcomes remain unclear. Future research, including an individual patient data meta-analysis, could help clarify some of the observed findings in this updated systematic review.
现有的临床实践指南支持在急性呼吸窘迫综合征(ARDS)中使用神经肌肉阻滞剂(NMBA);然而,最近一项大型随机临床试验(RCT)对这种做法提出了质疑。因此,我们更新了之前的系统评价,以确定NMBA在ARDS中的疗效和安全性。
我们检索了MEDLINE、EMBASE(2012年10月至2019年7月)、Cochrane(Central)数据库以及临床试验注册库(ClinicalTrials.gov、ISRCTN注册库和世界卫生组织国际临床试验平台),以查找比较NMBA持续输注与安慰剂或不输注NMBA(但允许间歇性NMBA推注)对ARDS成年患者重要结局影响的RCT。两名独立的评审员评估了主要研究的方法学质量并提取了数据。
七项RCT,包括四项新的RCT,符合本评价的纳入标准。这些试验在美国、法国和中国的中心纳入了1598例中重度ARDS患者。所有试验均评估了顺式阿曲库铵或维库溴铵的短期持续输注。死亡率结局的汇总估计显示出显著的统计学异质性,这仅通过对照臂镇静深度的亚组分析得到了解释。与不进行NMBA输注的轻度镇静策略相比,持续输注NMBA并未改善死亡率(相对风险[RR]0.99;95%CI 0.86-1.15;中等确定性;P = 0.93)。另一方面,与根据需要进行NMBA推注的深度镇静相比,持续输注NMBA可降低死亡率(RR 0.71;95%CI 0.57-0.89;低确定性;P = 0.003)。在符合条件的试验中,持续输注NMBA降低了气压伤的发生率(RR 0.55;95%CI 0.35-0.85,中等确定性;P = 0.008),但对无呼吸机天数、机械通气时间和ICU获得性肌无力的影响尚不确定。
研究方法和结果的不一致性使得无法汇总所有试验的死亡率数据。在一项预先计划的敏感性分析中,NMBA输注对死亡率的影响取决于对照臂所采用的策略,与深度镇静相比死亡率降低,但与轻度镇静相比对死亡率无影响。在这两种情况下,持续输注NMBA可能会降低气压伤的风险,但对其他患者重要结局的影响仍不清楚。未来的研究,包括个体患者数据的荟萃分析,可能有助于阐明本更新系统评价中观察到的一些结果。