Institute of Pathology, University of Bern, Bern, Switzerland.
Department of Medical Oncology, Inselspital University Hospital Bern, Bern, Switzerland.
Mod Pathol. 2021 Jul;34(7):1333-1344. doi: 10.1038/s41379-021-00777-y. Epub 2021 Mar 13.
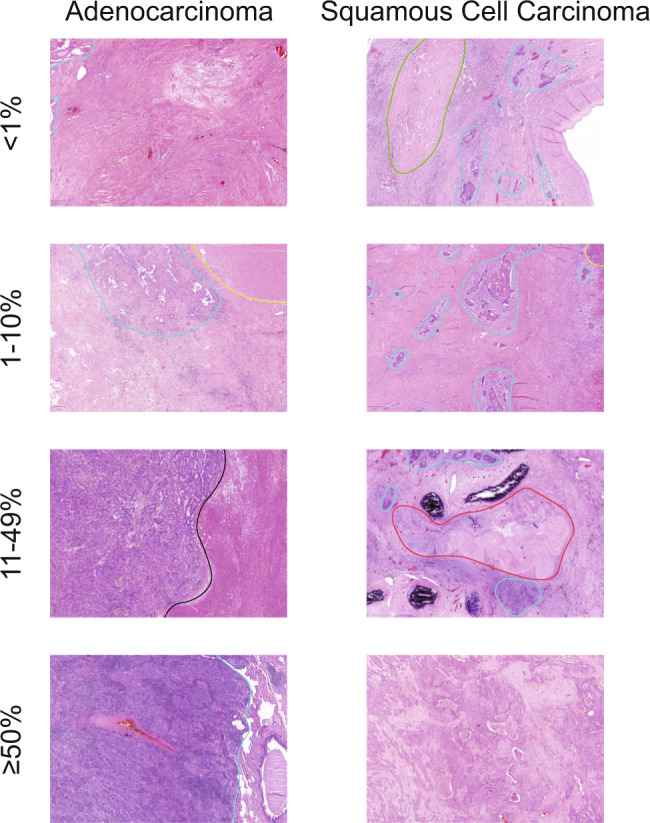
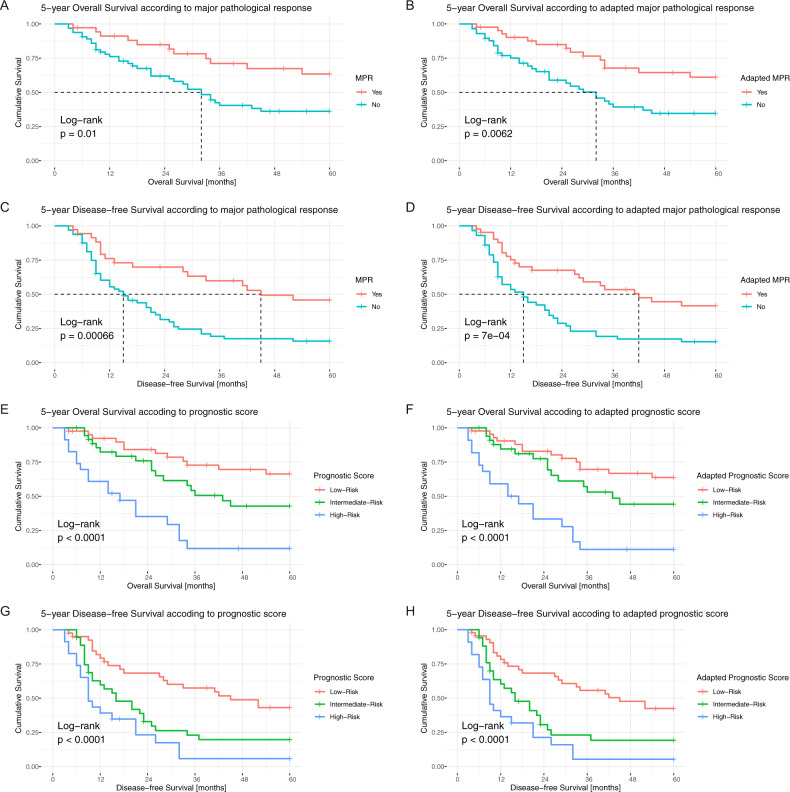
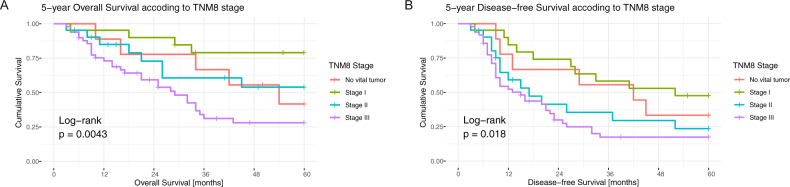
Studies validating the prognostic accuracy of the tumor-node-metastases (TNM) classification in patients with lung cancer treated by neoadjuvant therapy are scarce. Tumor regression, particularly major pathological response (MPR), is an acknowledged prognostic factor in this setting. We aimed to validate a novel combined prognostic score. This retrospective single-center study was conducted on 117 consecutive patients with non-small cell lung cancer resected after neoadjuvant treatment at a Swiss University Cancer Center between 2000 and 2016. All cases were clinicopathologically re-evaluated. We assessed the prognostic performance of a novel prognostic score (PRSC) combining T-category, lymph node status, and MPR, in comparison with the eighth edition of the TNM classification (TNM8), the size adapted TNM8 as proposed by the International Association for the Study of Lung Cancer (IASLC) and MPR alone. The isolated ypT-category and the combined TNM8 stages accurately differentiated overall survival (OS, stage p = 0.004) and disease-free survival (DFS, stage p = 0.018). Tumor regression had a prognostic impact. Optimal cut-offs for MPR emerged as 65% for adenocarcinoma and 10% for non-adenocarcinoma and were statistically significant for survival (OS p = 0.006, DFS p < 0.001). The PRSC differentiated between three prognostic groups (OS and DFS p < 0.001), and was superior compared to the stratification using MPR alone or the TNM8 systems, visualized by lower Akaike (AIC) and Bayesian information criterion (BIC) values. In the multivariate analyses, stage III tumors (HR 4.956, p = 0.003), tumors without MPR (HR 2.432, p = 0.015), and PRSC high-risk tumors (HR 5.692, p < 0.001) had significantly increased risks of occurring death. In conclusion, we support 65% as the optimal cut-off for MPR in adenocarcinomas. TNM8 and MPR were comparable regarding their prognostic significance. The novel prognostic score performed distinctly better regarding OS and DFS.
在接受新辅助治疗的肺癌患者中,验证肿瘤-淋巴结-转移(TNM)分类的预后准确性的研究很少。肿瘤退缩,特别是主要病理反应(MPR),是该情况下公认的预后因素。我们旨在验证一种新的联合预后评分。这项回顾性单中心研究于 2000 年至 2016 年在瑞士大学癌症中心对 117 例接受新辅助治疗后切除的非小细胞肺癌患者进行。所有病例均进行了临床病理再评估。我们评估了一种新的预后评分(PRSC)结合 T 分期、淋巴结状态和 MPR 的预后性能,与第八版 TNM 分类(TNM8)、国际肺癌研究协会(IASLC)提出的大小适应的 TNM8 以及单独的 MPR 进行比较。孤立的 ypT 分期和联合的 TNM8 分期准确地区分了总生存期(OS,分期 p=0.004)和无病生存期(DFS,分期 p=0.018)。肿瘤退缩具有预后影响。腺癌的 MPR 最佳截断值为 65%,非腺癌为 10%,对生存具有统计学意义(OS p=0.006,DFS p<0.001)。PRSC 区分了三个预后组(OS 和 DFS p<0.001),并且与单独使用 MPR 或 TNM8 系统分层相比具有优越性,通过较低的 Akaike(AIC)和贝叶斯信息准则(BIC)值可视化。在多变量分析中,III 期肿瘤(HR 4.956,p=0.003)、无 MPR 的肿瘤(HR 2.432,p=0.015)和 PRSC 高危肿瘤(HR 5.692,p<0.001)发生死亡的风险显著增加。总之,我们支持 65%作为腺癌中 MPR 的最佳截断值。TNM8 和 MPR 在其预后意义方面具有可比性。新型预后评分在 OS 和 DFS 方面表现明显更好。