Division of Cardiology, Department of Medicine, Weill Cornell Medicine, New York, New York; Division of Cardiology, Department of Medicine, Columbia University Irving Medical Center, New York, New York.
Division of Cardiology, Department of Medicine, Weill Cornell Medicine, New York, New York.
J Am Soc Echocardiogr. 2021 Aug;34(8):839-850.e1. doi: 10.1016/j.echo.2021.03.002. Epub 2021 Mar 11.
Right ventricular hypertrophy (RVH) provides a key remodeling index alterable by pulmonary hypertension. Although echocardiography commonly integrates linear wall thickness and chamber dimensions to quantify left ventricular remodeling, the utility of an equivalent right ventricular (RV)-based approach is unknown.
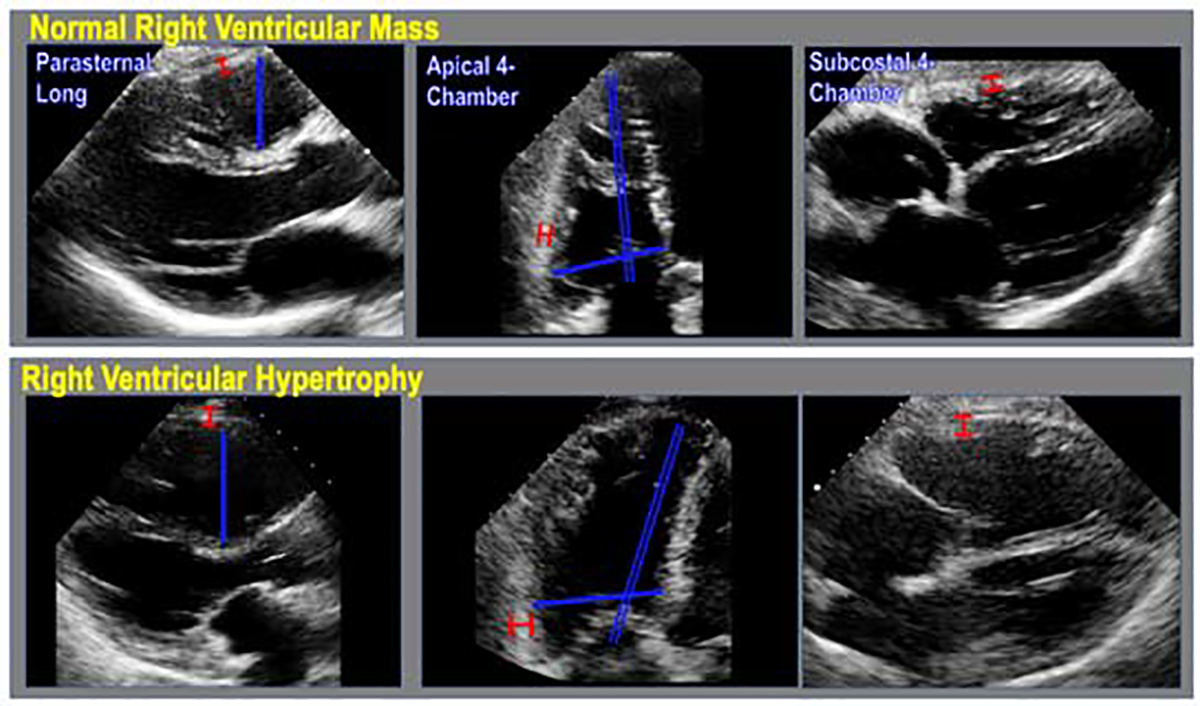
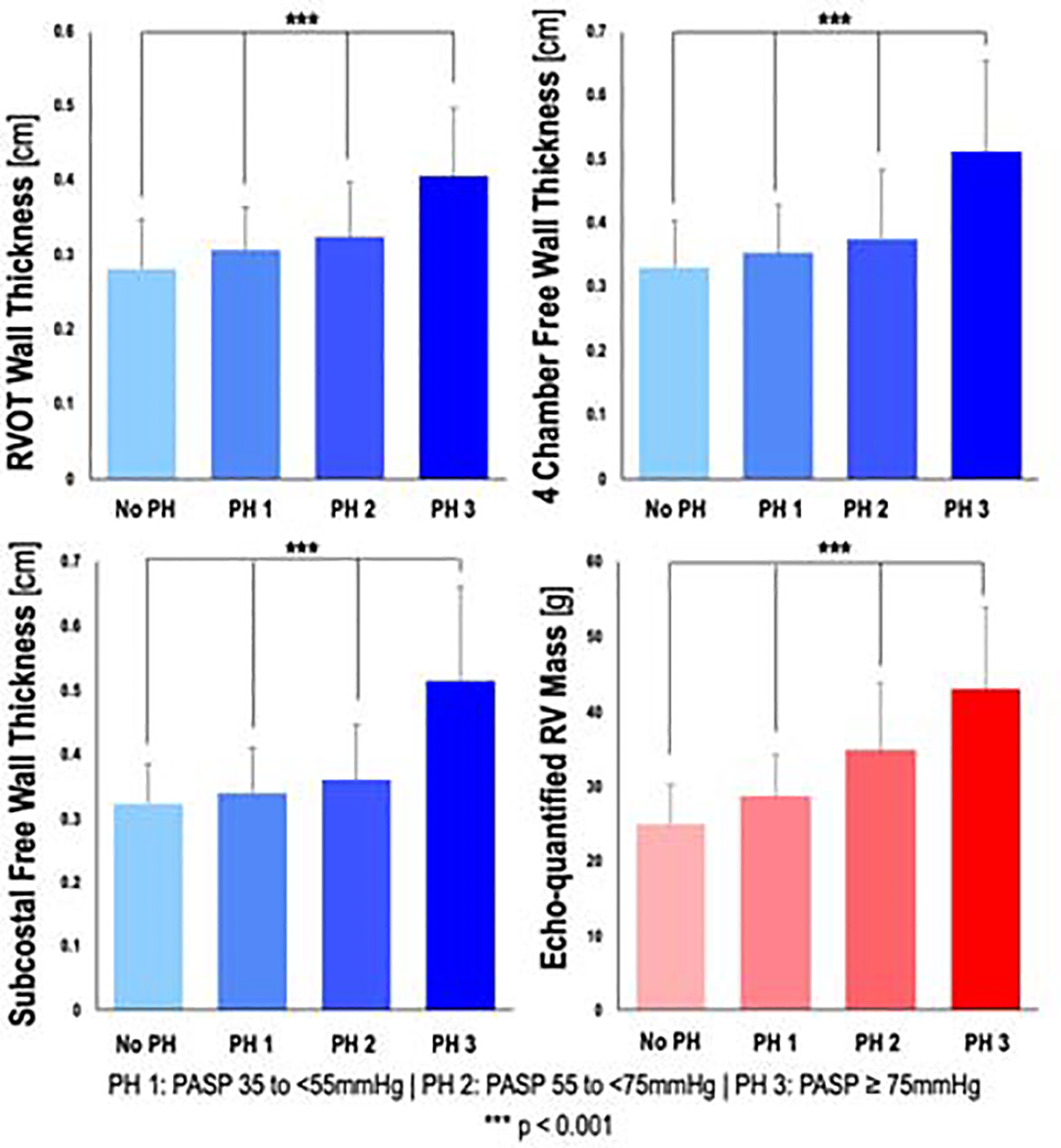
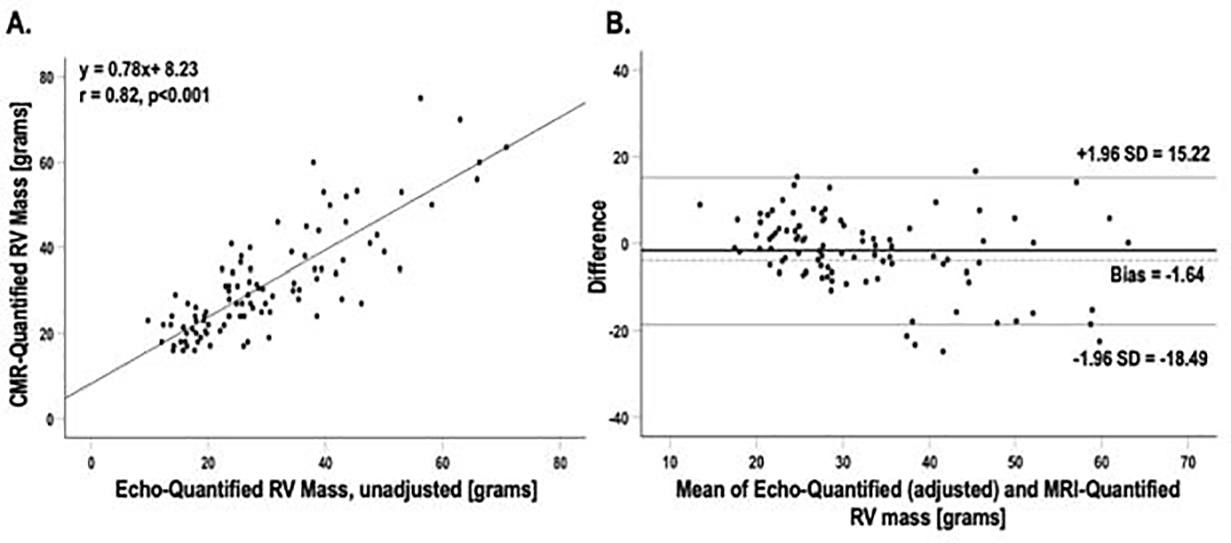
This was a retrospective analysis of 200 patients undergoing transthoracic echocardiography and cardiac magnetic resonance (CMR) within 30 days (median = 3 days; interquartile range, 15 days), stratified by echocardiography-quantified pulmonary artery systolic pressure (<35, 35 to <55, 55 to <75, or ≥75 mm Hg). Echocardiographic assessment included RV linear dimensions in parasternal long-axis and apical four-chamber views and wall thicknesses in parasternal long-axis, four-chamber, and subcostal views. Subcostal wall thickness was integrated with chamber diameters to calculate RV mass, which was tested in relation to CMR-quantified RV mass and all-cause mortality.
Echocardiography-based quantification of all linear dimensions was feasible in 95% of patients (190 of 200). RV wall thicknesses in all orientations increased in relation to pulmonary artery systolic pressure (P < .001) and was greater among patients with, versus those without, CMR-evidenced RVH (P < .001 for all). Correlations between echocardiography and CMR were greatest for RV basal diameter (r = 0.73), RV subcostal wall thickness (r = 0.71), and global RV mass (r = 0.82; P < .001 for all). Echocardiography-derived global RV mass cutoffs were established in a derivation cohort and tested in a validation cohort. Results demonstrated good sensitivity and specificity (75.5% and 74.0%, respectively) in relation to CMR-quantified RVH. During follow-up (median, 4.2 years), 18% of patients (n = 36) died. Echocardiography-evidenced RVH (hazard ratio, 1.98; 95% CI, 1.09-3.88; P = .048) conferred similar mortality risk compared with RVH on CMR (hazard ratio, 2.41; 95% CI, 1.22-4.78; P = .01).
Echocardiography-quantified RV parameters provide a robust index of RV afterload. Global RV mass calculated using a novel echocardiographic formula based on readily available linear indices yields good diagnostic performance for CMR-evidenced RVH and confers increased mortality risk.
右心室肥厚(RVH)是肺动脉高压后可改变的关键重构指标。虽然超声心动图通常将线性壁厚度和腔室尺寸整合起来量化左心室重构,但等效的右心室(RV)方法的实用性尚不清楚。
这是一项回顾性分析,纳入了 200 例在 30 天内(中位数=3 天;四分位距,15 天)接受经胸超声心动图和心脏磁共振(CMR)检查的患者,根据超声心动图量化的肺动脉收缩压(<35、35 至<55、55 至<75、或≥75mmHg)进行分层。超声心动图评估包括胸骨旁长轴和心尖四腔心切面的 RV 线性尺寸以及胸骨旁长轴、四腔心和肋下切面的壁厚度。肋下壁厚度与腔直径相结合计算 RV 质量,并在 CMR 量化的 RV 质量和全因死亡率方面进行了测试。
95%(200 例中有 190 例)的患者可行基于超声心动图的所有线性尺寸的定量评估。随着肺动脉收缩压的升高,所有方向的 RV 壁厚度均增加(P<.001),并且在 CMR 证实存在 RVH 的患者中大于不存在 RVH 的患者(所有 P<.001)。超声心动图与 CMR 之间的相关性以 RV 基底直径(r=0.73)、RV 肋下壁厚度(r=0.71)和整体 RV 质量(r=0.82;所有 P<.001)最大。在一个推导队列中建立了基于超声心动图的整体 RV 质量截断值,并在验证队列中进行了测试。结果表明,与 CMR 量化的 RVH 相比,该截断值具有良好的灵敏度和特异性(分别为 75.5%和 74.0%)。在随访期间(中位数为 4.2 年),18%(n=36)的患者死亡。超声心动图证实的 RVH(风险比,1.98;95%置信区间,1.09-3.88;P=.048)与 CMR 证实的 RVH(风险比,2.41;95%置信区间,1.22-4.78;P=.01)相比,具有相似的死亡风险。
超声心动图量化的 RV 参数提供了 RV 后负荷的可靠指标。使用基于线性指数的新超声心动图公式计算的整体 RV 质量对 CMR 证实的 RVH 具有良好的诊断性能,并增加了死亡风险。