Frangopoulos Frangiskos, Zannetos Savvas, Nicolaou Ivi, Economou Nicholas-Tiberio, Adamide Tonia, Georgiou Andreas, Nikolaidis Pantelis T, Rosemann Thomas, Knechtle Beat, Trakada Georgia
Respiratory Department, Nicosia General Hospital, Nicosia, Cyprus.
Health Economics and Statistics, Neapolis University, Paphos, Cyprus.
Front Psychiatry. 2021 Feb 25;12:630162. doi: 10.3389/fpsyt.2021.630162. eCollection 2021.
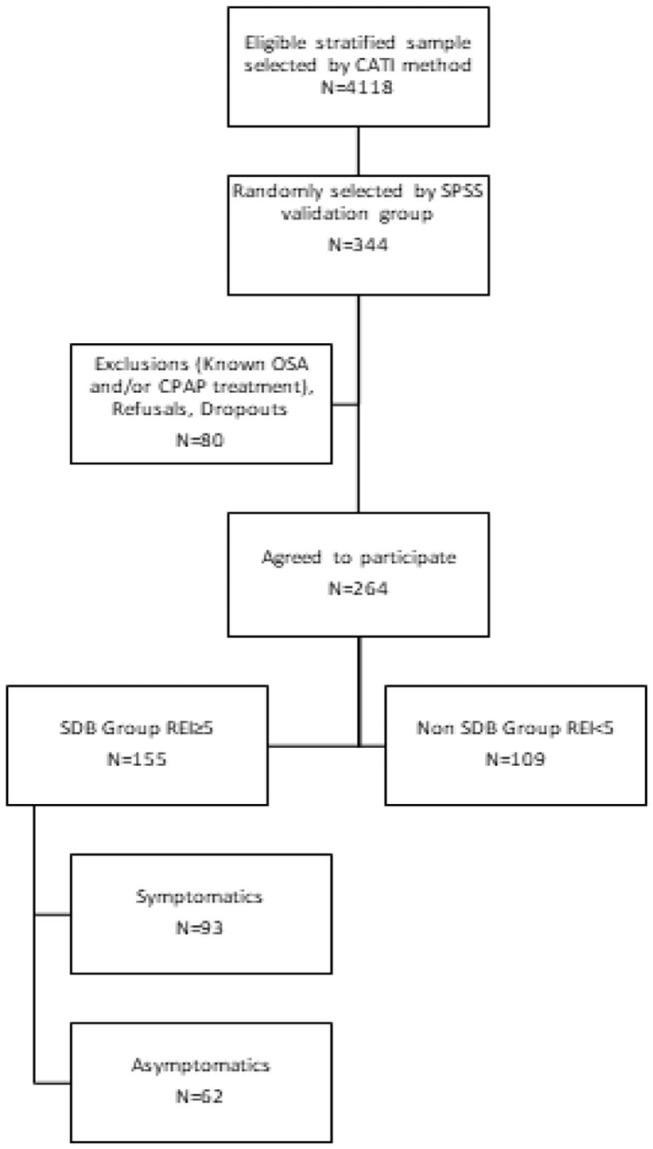
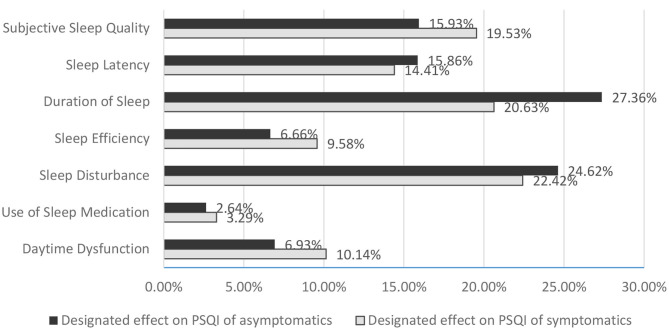
Little information exists in the general population whether clinical presentation phenotypes of obstructive sleep apnea (OSA) differ in terms of sleep quality and comorbidities. The purpose of our study was to assess possible differences between symptomatic and asymptomatic OSA patients concerning syndrome's severity, patients' sleep quality, and comorbidities. First, in a nationwide, stratified, epidemiological survey, 4,118 Cypriot adult participants were interviewed about sleep habits and complaints. In the second stage of the survey, 264 randomly selected adults underwent a type III sleep study for possible OSA. Additionally, they completed the Greek version of Pittsburgh Sleep Quality Index (Gr-PSQI), Epworth Sleepiness Scale (ESS), Athens Insomnia Scale (AIS), and Hospital Anxiety and Depression Scale (HADS). From 264 enrolled participants, 155 individuals (40 females and 115 males) were first diagnosed with OSA. Among these 155 patients, 34% had ESS ≥ 10 and 49% AIS ≥ 6. One or both symptoms present categorized the individual as symptomatic (60%) and neither major symptom as asymptomatic (40%). There were no significant statistical differences (SSDs) between the two groups (symptomatic-asymptomatic) with regard to anthropometrics [age or gender; neck, abdomen, and hip circumferences; and body mass index (BMI)]. The two groups had no differences in OSA severity-as expressed by apnea-hypopnea index (AHI), oxygen desaturation index (ODI), and mean oxyhemoglobin saturation (SaO)-and in cardiometabolic comorbidities. Symptomatic patients expressed anxiety and depression more often than asymptomatics ( < 0.001) and had poorer subjective sleep quality (Gr-PSQI, < 0.001). According to PSQI questionnaire, there were no SSDs regarding hours in bed and the use of sleep medications, but there were significant differences in the subjective perception of sleep quality ( < 0.001), sleep efficiency ( < 0.001), duration of sleep ( = 0.001), sleep latency ( = 0.007), daytime dysfunction ( < 0.001), and finally sleep disturbances ( < 0.001). According to our data, OSA patients reporting insomnia-like symptoms and/or sleepiness do not represent a more severe phenotype, by the classic definition of OSA, but their subjective sleep quality is compromised, causing a vicious cycle of anxiety or depression.
普通人群中关于阻塞性睡眠呼吸暂停(OSA)的临床表现型在睡眠质量和合并症方面是否存在差异的信息很少。我们研究的目的是评估有症状和无症状的OSA患者在综合征严重程度、患者睡眠质量和合并症方面可能存在的差异。首先,在一项全国性的分层流行病学调查中,对4118名塞浦路斯成年参与者进行了关于睡眠习惯和睡眠问题的访谈。在调查的第二阶段,264名随机选择的成年人接受了III型睡眠研究以排查可能的OSA。此外,他们完成了希腊版的匹兹堡睡眠质量指数(Gr-PSQI)、爱泼沃斯嗜睡量表(ESS)、雅典失眠量表(AIS)和医院焦虑抑郁量表(HADS)。在264名登记参与者中,155人(40名女性和115名男性)首次被诊断为OSA。在这155名患者中,34%的人ESS≥10,49%的人AIS≥6。存在一种或两种症状的个体被归类为有症状(60%),没有主要症状的个体被归类为无症状(40%)。两组(有症状-无症状)在人体测量学指标[年龄或性别;颈部、腹部和臀部周长;以及体重指数(BMI)]方面没有显著统计学差异(SSD)。两组在以呼吸暂停低通气指数(AHI)、氧饱和度下降指数(ODI)和平均氧合血红蛋白饱和度(SaO)表示的OSA严重程度以及心脏代谢合并症方面没有差异。有症状的患者比无症状的患者更常表现出焦虑和抑郁(<0.001),并且主观睡眠质量较差(Gr-PSQI,<0.001)。根据PSQI问卷,在床上的时间和使用助眠药物方面没有SSD,但在睡眠质量的主观感受(<0.001)、睡眠效率(<0.001)、睡眠时间(=0.001)、入睡潜伏期(=0.007)、日间功能障碍(<0.001)以及最终的睡眠障碍(<0.001)方面存在显著差异。根据我们的数据,报告有失眠样症状和/或嗜睡的OSA患者,按照OSA的经典定义,并不代表更严重的表型,但他们的主观睡眠质量受到损害,导致焦虑或抑郁的恶性循环。