Medical Oncology Unit, Department of Medical and Surgical Specialties, Radiological Sciences and Public Health, University of Brescia at ASST Spedali Civili, Brescia, Italy.
Radiology Unit, Azienda Socio Sanitaria Territoriale (ASST) Spedali Civili, Brescia, Italy.
Front Endocrinol (Lausanne). 2021 Feb 24;12:624102. doi: 10.3389/fendo.2021.624102. eCollection 2021.
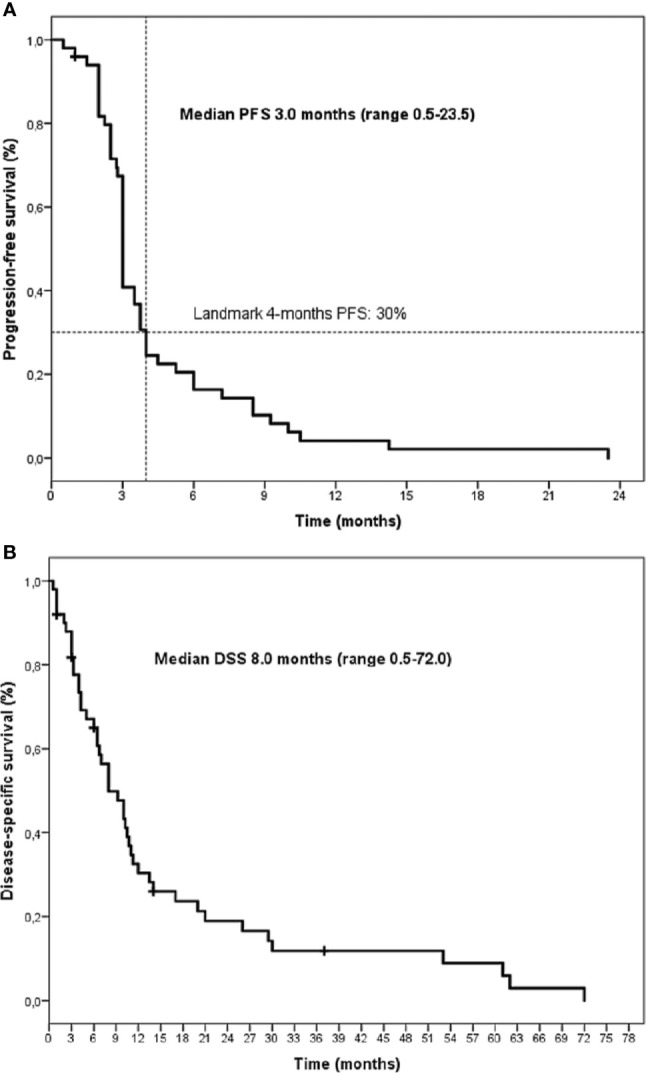
Gemcitabine plus Capecitabine (Gem/Cape) is a frequently adopted second line chemotherapy for metastatic adrenocortical carcinoma (ACC), but only a minority of patients is destined to obtain a clinical benefit. The identification of baseline predictive factors of efficacy is relevant. We retrospectively analyzed clinical data from 50 consecutive patients with metastatic progressing ACC treated between 2011 and 2019. Patients received intravenous Gemcitabine and oral Capecitabine on a metronomic schedule. Previous mitotane therapy was maintained. Clinical benefit (partial response + stable disease) at 4 months was 30%, median progression-free survival (PFS) and disease-specific survival (DSS) from Gem/Cape start were 3 and 8 months, respectively. Among clinical variables evaluated before the start of Gem/Cape, presence of ECOG performance status ≥1 [HR 6.93 95% confidence interval (CI) 0.03-0.54, p.004] and neutrophil-to-lymphocyte ratio (NLR) ≥5 [HR 3.88, 95% (CI) 0.81-0.90, p.003] were independent indicators of poor PFS at multivariate analysis. Conversely, surgery of primary tumor, the presence of lung or lymph-node metastases, blood mitotane level, anemia, and the Advanced Lung cancer Inflammation index (ALI) failed to be independently associated. This study confirms that the Gem/Cape schedule is modestly active in heavily pretreated ACC patients (28% received at least two previous chemotherapy lines). NLR and performance status (PS) are easily available clinical parameters that are helpful to identify patients not likely to derive significant advantage from Gem/Cape chemotherapy.
吉西他滨联合卡培他滨(Gem/Cape)是转移性肾上腺皮质癌(ACC)常用的二线化疗方案,但只有少数患者能从中获得临床获益。因此,明确疗效的基线预测因素非常重要。我们回顾性分析了 2011 年至 2019 年期间 50 例转移性进展期 ACC 患者的临床资料。患者接受静脉注射吉西他滨和口服卡培他滨的节拍式化疗方案,同时维持米托坦治疗。以 4 个月时的临床获益(部分缓解+疾病稳定)作为评价疗效的指标,Gem/Cape 起始后中位无进展生存期(PFS)和疾病特异性生存期(DSS)分别为 3 个月和 8 个月。在开始 Gem/Cape 前评估的临床变量中,ECOG 体能状态评分≥1[风险比(HR)6.93,95%置信区间(CI)0.03-0.54,p.004]和中性粒细胞与淋巴细胞比值(NLR)≥5[HR 3.88,95%CI 0.81-0.90,p.003]是多因素分析中 PFS 较差的独立预测因素。而肿瘤手术、肺或淋巴结转移、血中米托坦浓度、贫血和肺癌炎症指数(ALI)均不能独立预测。本研究证实,在经过大量预处理的 ACC 患者中,Gem/Cape 方案具有一定的疗效(28%的患者至少接受过两种先前的化疗方案)。NLR 和体能状态(PS)是两种易于获得的临床参数,有助于识别不能从 Gem/Cape 化疗中获益的患者。