Department of Science and Innovation - National Research Foundation (DSI-NRF) Centre of Excellence for Biomedical Tuberculosis Research, South African Medical Research Council Centre for Tuberculosis Research, Division of Molecular Biology and Human Genetics, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa.
TB Research Group, Medical Research Council Gambia at London School of Hygiene and Tropical Medicine (LSHTM), Banjul, Gambia.
Front Immunol. 2021 Feb 26;12:607827. doi: 10.3389/fimmu.2021.607827. eCollection 2021.
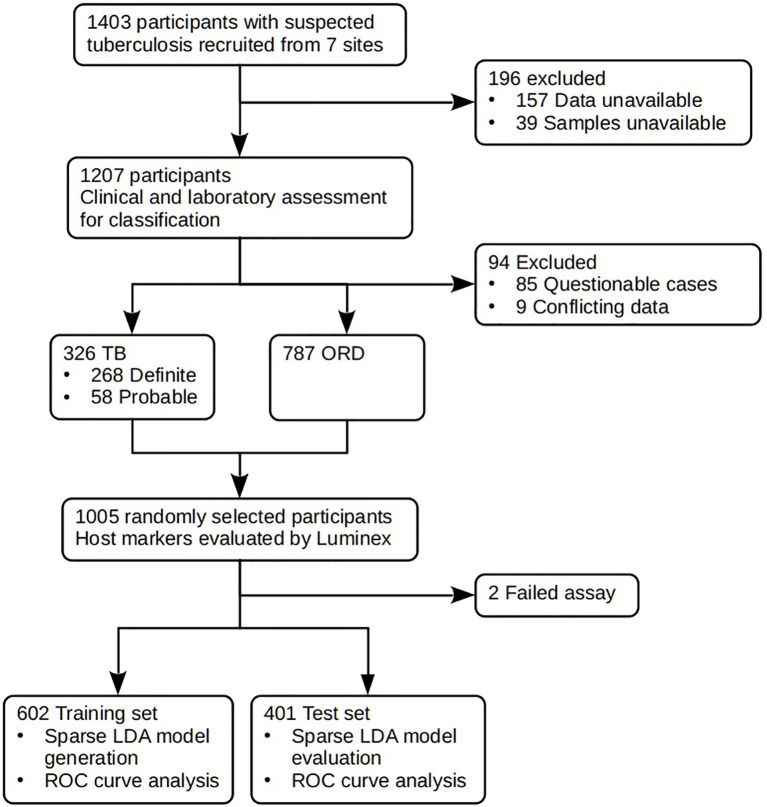
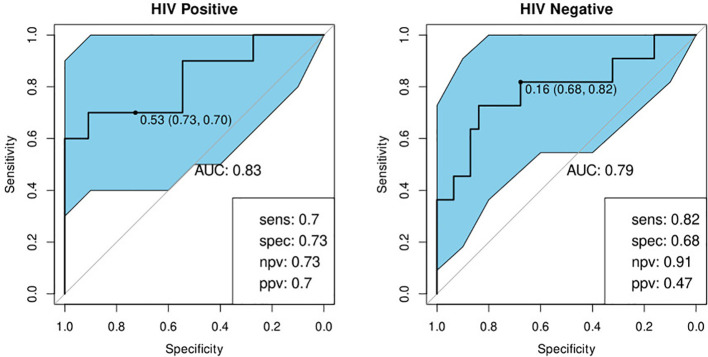
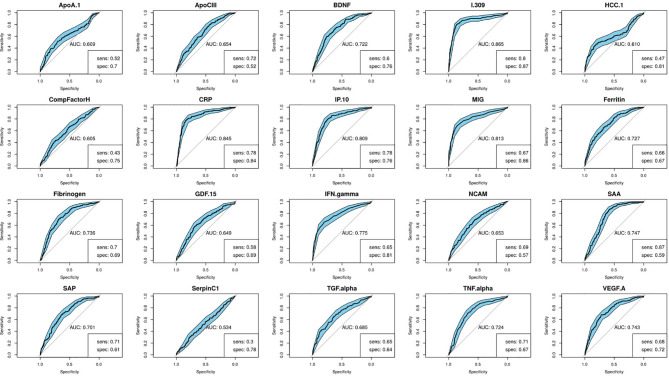
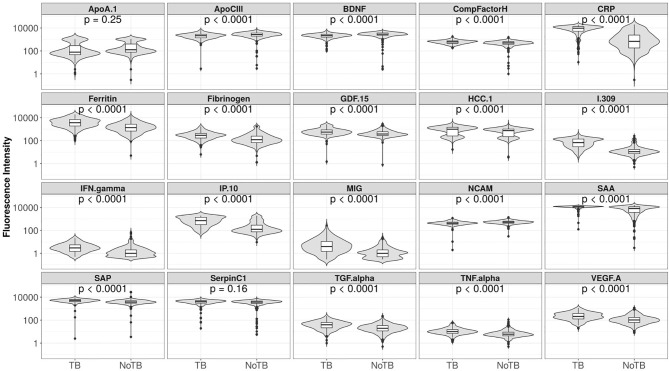
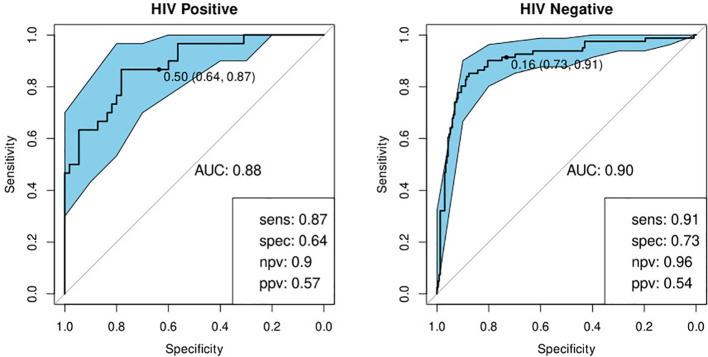
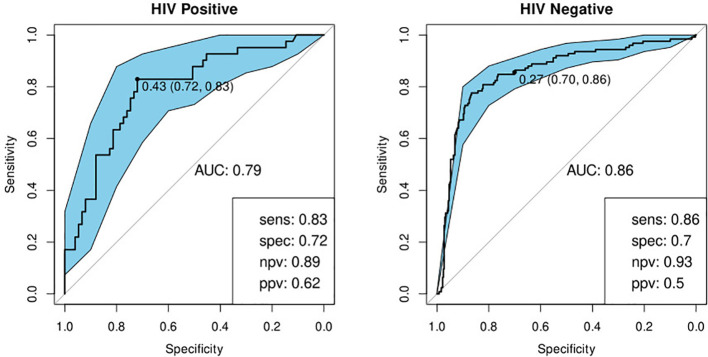
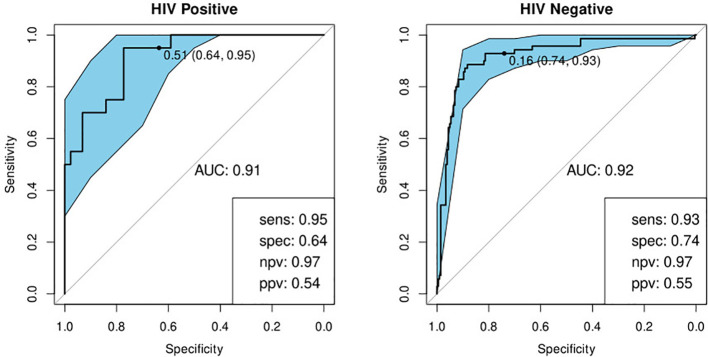
The development of a non-sputum-based, point-of-care diagnostic test for tuberculosis (TB) is a priority in the global effort to combat this disease, particularly in resource-constrained settings. Previous studies have identified host biomarker signatures which showed potential, but there is a need to validate and refine these for development as a test. We recruited 1,403 adults presenting with symptoms suggestive of pulmonary TB at primary healthcare clinics in six countries from West, East and Southern Africa. Of the study cohort, 326 were diagnosed with TB and 787 with other respiratory diseases, from whom we randomly selected 1005 participants. Using Luminex technology, we measured the levels of 20 host biomarkers in serum samples which we used to evaluate the diagnostic accuracy of previously identified and novel bio-signatures. Our previously identified seven-marker bio-signature did not perform well (sensitivity: 89%, specificity: 60%). We also identified an optimal, two-marker bio-signature with a sensitivity of 94% and specificity of 69% in patients with no history of previous TB. This signature performed slightly better than C-reactive protein (CRP) alone. The cut-off value for a positive diagnosis differed for human immuno-deficiency virus (HIV)-positive and -negative individuals. Notably, we also found that no signature was able to diagnose TB adequately in patients with a prior history of the disease. We have identified a two-marker, pan-African bio-signature which is more robust than CRP alone and meets the World Health Organization (WHO) target product profile requirements for a triage test in both HIV-negative and HIV-positive individuals. This signature could be incorporated into a point-of-care device, greatly reducing the necessity for expensive confirmatory diagnostics and potentially reducing the number of cases currently lost to follow-up. It might also potentially be useful with individuals unable to provide sputum or with paucibacillary disease. We suggest that the performance of TB diagnostic signatures can be improved by incorporating the HIV-status of the patient. We further suggest that only patients who have never had TB be subjected to a triage test and that those with a history of previous TB be evaluated using more direct diagnostic techniques.
开发一种基于非痰液、即时检测的结核病(TB)诊断测试是全球抗击这种疾病的重点,特别是在资源有限的环境中。先前的研究已经确定了宿主生物标志物特征,这些特征显示出了潜力,但需要对其进行验证和改进,以开发成为一种测试。我们招募了来自西非、东非和南非的六个国家的初级保健诊所中出现疑似肺结核症状的 1403 名成年人。在研究队列中,326 人被诊断为结核病,787 人被诊断为其他呼吸道疾病,我们从这些人中随机选择了 1005 名参与者。使用 Luminex 技术,我们测量了血清样本中 20 种宿主生物标志物的水平,用于评估先前确定的和新的生物标志物的诊断准确性。我们之前确定的七标志物生物标志物表现不佳(敏感性:89%,特异性:60%)。我们还确定了一种最佳的、两种标志物生物标志物,在没有既往结核病史的患者中具有 94%的敏感性和 69%的特异性。该标志物的性能略优于单独的 C 反应蛋白(CRP)。阳性诊断的截止值因人类免疫缺陷病毒(HIV)阳性和阴性个体而异。值得注意的是,我们还发现,对于既往患有该病的患者,没有任何标志物能够充分诊断结核病。我们已经确定了一种泛非的、由两种标志物组成的生物标志物,它比单独的 CRP 更可靠,并且符合世界卫生组织(WHO)对用于 HIV 阴性和 HIV 阳性个体的分诊测试的目标产品概况要求。这种标志物可以被纳入即时检测设备中,极大地减少了对昂贵的确认性诊断的需求,并可能减少目前因无法随访而导致的病例数量。对于无法提供痰液或仅有少量细菌的患者,它也可能具有潜在的作用。我们建议通过纳入患者的 HIV 状态来提高 TB 诊断标志物的性能。我们进一步建议,只有从未患过结核病的患者才需要进行分诊测试,而对于有既往结核病病史的患者,则应使用更直接的诊断技术进行评估。