Division of Infection and Immunity, University College London, London, UK.
Institute for Global Health, University College London, London, UK.
Lancet Respir Med. 2020 Apr;8(4):407-419. doi: 10.1016/S2213-2600(19)30469-2. Epub 2020 Mar 13.
Blood transcriptional signatures are candidates for non-sputum triage or confirmatory tests of tuberculosis. Prospective head-to-head comparisons of their diagnostic accuracy in real-world settings are necessary to assess their clinical use. We aimed to compare the diagnostic accuracy of candidate transcriptional signatures identified by systematic review, in a setting with a high burden of tuberculosis and HIV.
We did a prospective observational study nested within a diagnostic accuracy study of sputum Xpert MTB/RIF (Xpert) and Xpert MTB/RIF Ultra (Ultra) tests for pulmonary tuberculosis. We recruited consecutive symptomatic adults aged 18 years or older self-presenting to a tuberculosis clinic in Cape Town, South Africa. Participants provided blood for RNA sequencing, and sputum samples for liquid culture and molecular testing using Xpert and Ultra. We assessed the diagnostic accuracy of candidate blood transcriptional signatures for active tuberculosis (including those intended to distinguish active tuberculosis from other diseases) identified by systematic review, compared with culture or Xpert MTB/RIF positivity as the standard reference. In our primary analysis, patients with tuberculosis were defined as those with either a positive liquid culture or Xpert result. Patients with missing blood RNA or sputum results were excluded. Our primary objective was to benchmark the diagnostic accuracy of candidate transcriptional signatures against the WHO target product profile (TPP) for a tuberculosis triage test.
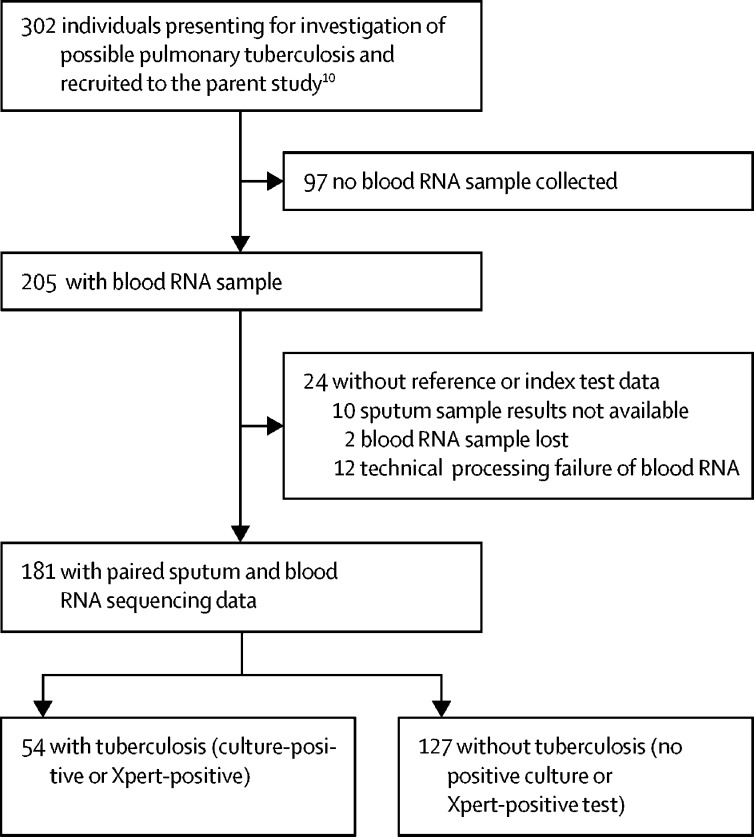
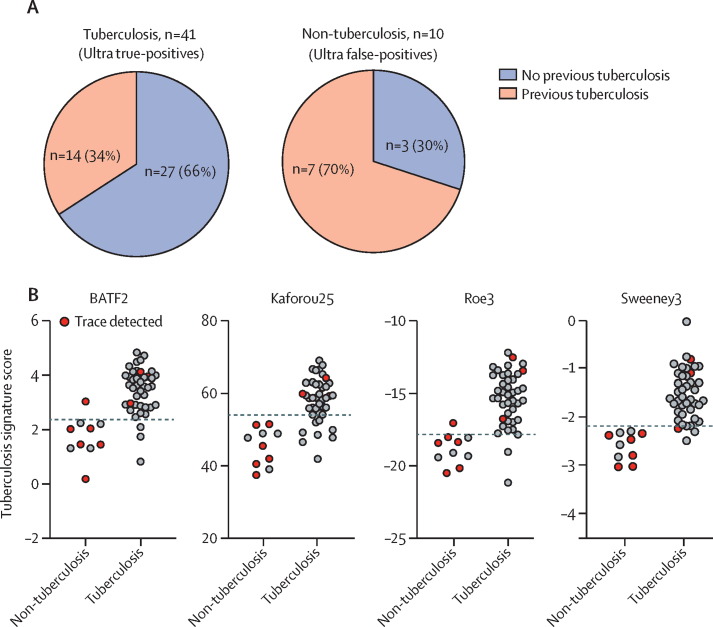
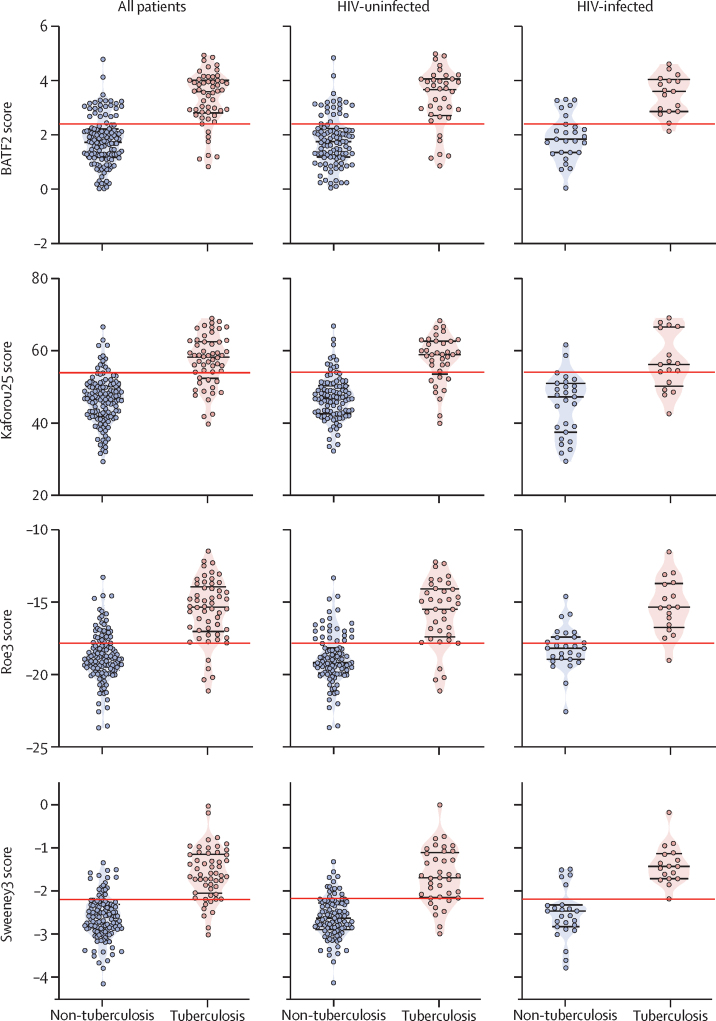
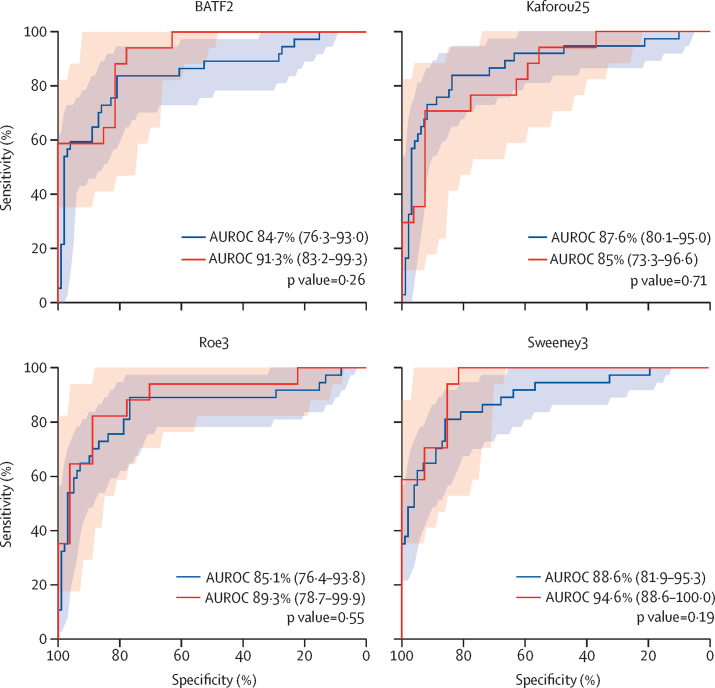
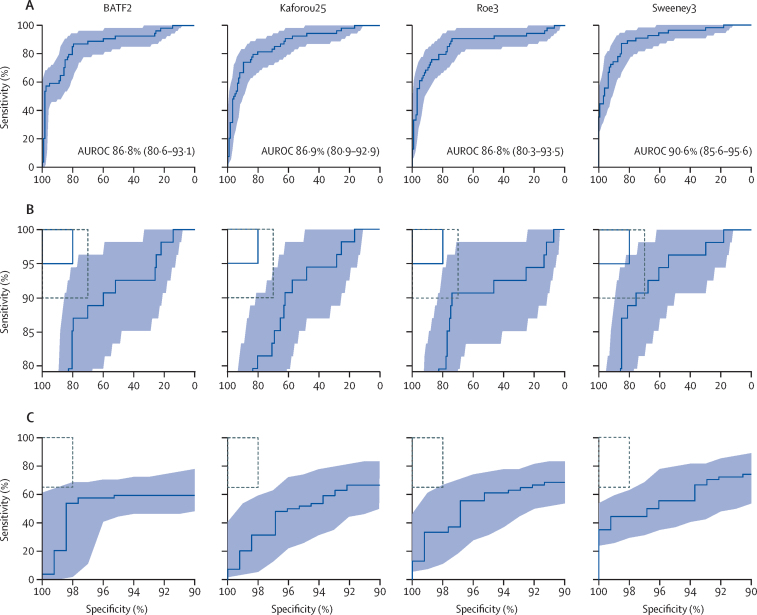
Between Feb 12, 2016, and July 18, 2017, we obtained paired sputum and RNA sequencing data from 181 participants, 54 (30%) of whom had confirmed pulmonary tuberculosis. Of 27 eligible signatures identified by systematic review, four achieved the highest diagnostic accuracy with similar area under the receiver operating characteristic curves (Sweeney3: 90·6% [95% CI 85·6-95·6]; Kaforou25: 86·9% [80·9-92·9]; Roe3: 86·9% [80·3-93·5]; and BATF2: 86·8% [80·6-93·1]), independent of age, sex, HIV status, previous tuberculosis, or sputum smear result. At test thresholds that gave 70% specificity (the minimum WHO TPP specificity for a triage test), these four signatures achieved sensitivities between 83·3% (95% CI 71·3-91·0) and 90·7% (80·1-96·0). No signature met the optimum criteria, of 95% sensitivity and 80% specificity proposed by WHO for a triage test, or the minimum criteria (of 65% sensitivity and 98% specificity) for a confirmatory test, but all four correctly identified Ultra-positive, culture-negative patients.
Selected blood transcriptional signatures met the minimum WHO benchmarks for a tuberculosis triage test but not for a confirmatory test. Further development of the signatures is warranted to investigate their possible effects on clinical and health economic outcomes as part of a triage strategy, or when used as add-on confirmatory test in conjunction with the highly sensitive Ultra test for Mycobacterium tuberculosis DNA.
Royal Society Newton Advanced Fellowship, Wellcome Trust, National Institute of Health Research, and UK Medical Research Council.
血液转录特征可作为结核病非痰标本初筛或确证检测的候选指标。为评估其临床应用价值,有必要在真实环境中对这些候选指标的诊断准确性进行前瞻性头对头比较。本研究旨在比较通过系统评价鉴定的候选转录特征在高结核和 HIV 负担环境中的诊断准确性。
我们开展了一项前瞻性观察性研究,嵌套在一项针对 Xpert MTB/RIF(Xpert)和 Xpert MTB/RIF Ultra(Ultra)检测的肺结核诊断准确性研究中。我们招募了自感症状的连续成年患者,年龄在 18 岁及以上,来自南非开普敦的一家结核病诊所。参与者提供血液进行 RNA 测序,并提供痰液样本进行液体培养和分子检测,包括 Xpert 和 Ultra。我们评估了系统评价鉴定的候选血液转录特征对活动性肺结核(包括用于区分活动性肺结核与其他疾病的特征)的诊断准确性,以培养或 Xpert MTB/RIF 阳性作为标准参考。在我们的主要分析中,将结核病患者定义为液体培养或 Xpert 结果阳性的患者。排除血液 RNA 或痰液结果缺失的患者。我们的主要目标是将候选转录特征的诊断准确性与世界卫生组织(WHO)的结核病筛查检测的目标产品特性(TPP)进行基准比较。
2016 年 2 月 12 日至 2017 年 7 月 18 日,我们从 181 名参与者中获得了配对的痰液和 RNA 测序数据,其中 54 名(30%)确诊为肺结核。在系统评价中确定的 27 个有资格的特征中,有 4 个特征具有相似的接收者操作特征曲线下面积(Sweeney3:90.6%[95%CI 85.6-95.6];Kaforou25:86.9%[80.9-92.9];Roe3:86.9%[80.3-93.5];和 BATF2:86.8%[80.6-93.1]),与年龄、性别、HIV 状态、既往结核病或痰涂片结果无关。在达到 70%特异性(WHO 对筛查检测的最低特异性)的检测阈值时,这 4 个特征的敏感性分别为 83.3%(95%CI 71.3-91.0)和 90.7%(80.1-96.0)。没有一个特征符合 WHO 提出的筛查检测的最佳标准(敏感性 95%,特异性 80%)或确认检测的最低标准(敏感性 65%,特异性 98%),但所有 4 个特征都正确识别了 Ultra 阳性、培养阴性的患者。
选定的血液转录特征符合 WHO 对结核病筛查检测的最低标准,但不符合确认检测的标准。需要进一步开发这些特征,以研究它们作为一种分诊策略的潜在临床和健康经济效益,或者作为与高度敏感的 Ultra 检测联合使用的附加确认检测,用于检测结核分枝杆菌 DNA。
英国皇家学会牛顿高级研究员基金、惠康信托基金、英国国家卫生研究院和英国医学研究理事会。