Dalakas Marinos C, Spaeth Peter J
Thomas Jefferson University, 900 Walnut Street, Philadelphia, PA 19107, USA.
Institute of Pharmacology, University of Bern, Bern, Switzerland.
Ther Adv Neurol Disord. 2021 Feb 26;14:1756286421997381. doi: 10.1177/1756286421997381. eCollection 2021.
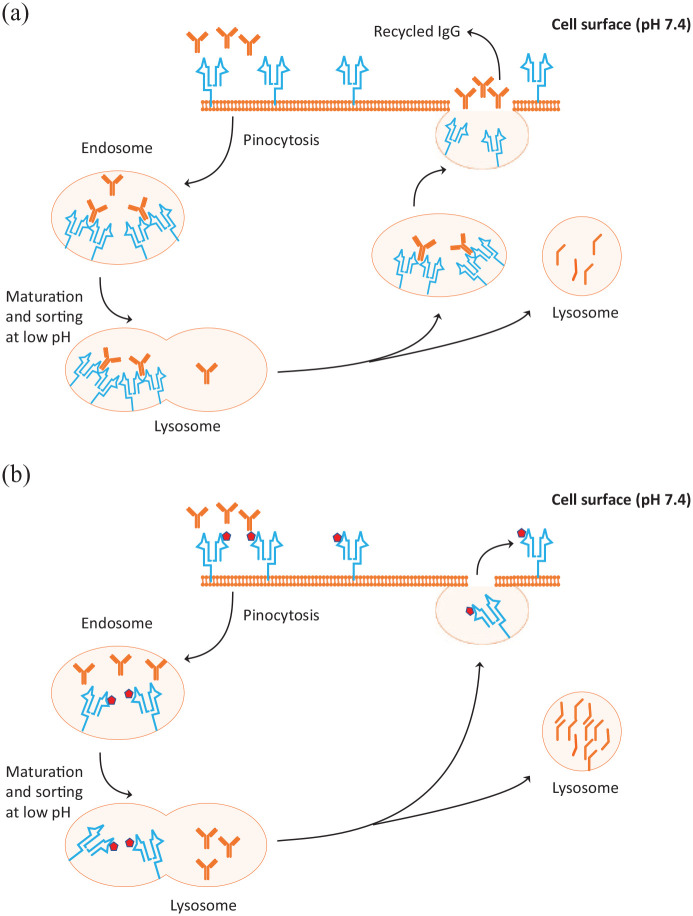
The neonatal Fc receptor (FcRn) binds endogenous IgG and protects it from lysosomal degradation by transporting it back to the cell surface to re-enter the circulation, extending the serum IgG life span. FcRn plays a role in the function of IVIg because the supraphysiological IgG levels derived from IVIg administrations saturate the FcRn allowing the endogenous IgG to be degraded, instead of being recycled, resulting in high levels of infused IgG ensuring IVIg efficiency. New data in myasthenia gravis patients suggest that the that the Variable Number of Tandem 3/2 (VNTR3/2) polymorphisms in , the gene that encodes FcRn, may affect the duration of infused IgG in the circulation and IVIg effectiveness. This review addresses these implications in the context of whether the genotype, by affecting the half-life of IVIg, may also play a role in up to 30% of patients with autoimmune neurological diseases, such as Guillain-Barré syndrome, CIDP or Multifocal Motor Neuropathy, who did not respond to IVIg in controlled trials. The concern is of practical significance because in such patient subsets super-high IVIg doses may be needed to achieve high IgG levels and ensure efficacy. Whether polymorphisms affect the efficacy of other therapeutic monoclonal antibodies by influencing their distribution clearance and pharmacokinetics, explaining their variable effectiveness, is also addressed. Finally, the very promising effect of monoclonal antibodies that inhibit FcRn, such as efgartigimod, rozanolixizumab and nipocalimab, in treating antibody-mediated neurological diseases is discussed along with their efficacy in the IgG4 subclass of pathogenic antibodies and their role in the blood-brain barrier endothelium, that abundantly expresses FcRn.
新生儿Fc受体(FcRn)可结合内源性IgG,并通过将其转运回细胞表面以重新进入循环,保护其免受溶酶体降解,从而延长血清IgG的寿命。FcRn在静脉注射免疫球蛋白(IVIg)的功能中发挥作用,因为IVIg给药产生的超生理水平IgG会使FcRn饱和,从而使内源性IgG被降解而非循环利用,从而确保高剂量注入的IgG能保证IVIg的疗效。重症肌无力患者的新数据表明,编码FcRn的基因中可变串联重复序列3/2(VNTR3/2)多态性可能会影响注入的IgG在循环中的持续时间以及IVIg的有效性。本综述探讨了在对照试验中对IVIg无反应的高达30%的自身免疫性神经疾病患者(如吉兰-巴雷综合征、慢性炎性脱髓鞘性多发性神经根神经病或多灶性运动神经病)中,该基因型是否通过影响IVIg的半衰期也发挥作用这一问题。这一问题具有实际意义,因为在这类患者亚组中,可能需要超高剂量的IVIg才能达到高IgG水平并确保疗效。还探讨了多态性是否通过影响其他治疗性单克隆抗体的分布清除和药代动力学来影响其疗效,从而解释其疗效差异。最后,讨论了抑制FcRn的单克隆抗体(如艾加莫德、罗扎诺利昔单抗和尼波卡利单抗)在治疗抗体介导的神经疾病方面非常有前景的效果,以及它们在致病性抗体的IgG4亚类中的疗效及其在大量表达FcRn的血脑屏障内皮中的作用。