Perek Bartlomiej, Olasinska-Wisniewska Anna, Misterski Marcin, Puslecki Mateusz, Grygier Marek, Buczkowski Piotr, Lesiak Maciej, Stankowski Tomasz, Szarpak Lukasz, Ruetzler Kurt, Turan Oguz, Jemielity Marek
Department of Cardiac Surgery and Transplantology, Poznan University of Medical Sciences, Poznan, Poland.
Department of Medical Rescue, Poznan University of Medical Sciences, Poznan, Poland.
J Thorac Dis. 2021 Feb;13(2):906-917. doi: 10.21037/jtd-20-3025.
Currently, two effective therapeutic options for severe aortic stenosis (AS) are available, one catheter-based [transcatheter aortic valve implantation (TAVI)], the other open surgical approach [surgical aortic valve replacement (SAVR)]. The COVID-19 pandemic has limited the availability of medical procedures. The purpose of this cross-sectional study was to assess if this pandemic had any impact on the treatment strategy of severe AS in a single cardiac center.
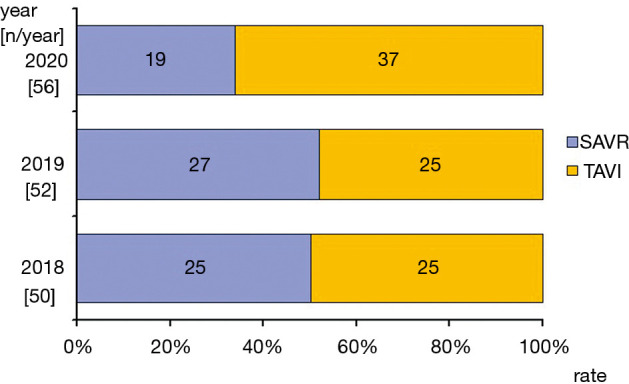
This study involved AS patients treated in 3-month periods (February through April) over 3 consecutive years 2018, 2019 [defined as COV(-) group] and 2020 [COV(+)]. We assessed if there were any differences regarding patients' clinical profile, applied therapeutic method, procedure complexity and early clinical outcomes.
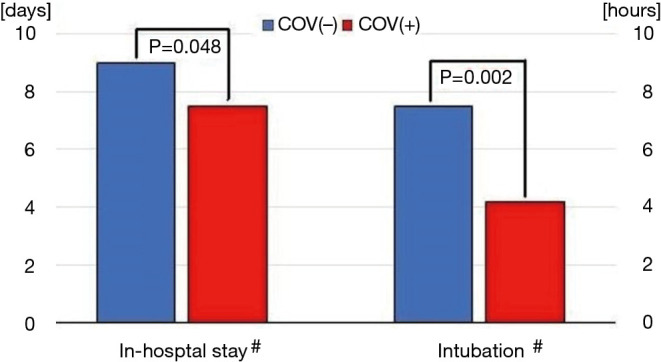
In the years 2018 through 2019, approximately 50% of AS patients were treated classically (SAVR) while in 2020 this rate dropped to 34%. The preoperative clinical characteristic of TAVI subjects was comparable irrespective of the year. Regarding SAVR, more patients in COV(+) underwent urgent and more complex procedures. More of them were found in NYHA class III or IV, and had lower left ventricular ejection fraction (LVEF) (51.9%±14.4% 58.3%±8.1%; P=0.021) than in COV(-) individuals. During the pandemic, a change in applied therapeutic methods and differences in patients' clinical profile did not have an unfavorable impact on in-hospital mortality (2.0% before 3.6% during pandemic) and morbidity. Of note, intubation time and in-hospital stay were significantly shorter (P<0.05) in 2020 (4.2 hours and 7.5 days) than in the previous years (7.5 hours and 9.0 days, respectively).
The coronavirus pandemic has changed substantially the management of severe AS. The shift into less invasive treatment method of AS patients resulted in shortening of in-hospital stay without compromise of short-term outcomes.
目前,重度主动脉瓣狭窄(AS)有两种有效的治疗选择,一种是基于导管的[经导管主动脉瓣植入术(TAVI)],另一种是开放手术方法[外科主动脉瓣置换术(SAVR)]。新型冠状病毒肺炎大流行限制了医疗程序的可及性。这项横断面研究的目的是评估这一大流行是否对单一心脏中心重度AS的治疗策略产生了任何影响。
本研究纳入了在2018年、2019年[定义为COV(-)组]和2020年[COV(+)]连续3年中每3个月期间(2月至4月)接受治疗的AS患者。我们评估了患者的临床特征、应用的治疗方法、手术复杂性和早期临床结果是否存在差异。
在2018年至2019年期间,约50%的AS患者接受传统治疗(SAVR),而在2020年这一比例降至34%。无论哪一年,TAVI受试者的术前临床特征具有可比性。对于SAVR,COV(+)组中更多患者接受了紧急且更复杂的手术。与COV(-)组个体相比,他们中更多患者处于纽约心脏协会(NYHA)Ⅲ或Ⅳ级,且左心室射血分数(LVEF)更低(分别为51.9%±14.4%和58.3%±8.1%;P=0.021)。在大流行期间,应用治疗方法的改变以及患者临床特征的差异对住院死亡率(大流行前为2.0%,大流行期间为3.6%)和发病率没有不利影响。值得注意的是,2020年的插管时间和住院时间(分别为4.2小时和7.5天)显著短于前几年(分别为7.5小时和9.0天)(P<0.05)。
新型冠状病毒大流行极大地改变了重度AS的管理。向AS患者采用侵入性较小的治疗方法转变导致住院时间缩短,而不影响短期结果。