Cheng Xueqing, Xu Jinshun, Chen Yuntian, Liu Zhenhua, Sun Guangxi, Yang Ling, Yao Jin, Zeng Hao, Song Bin
Department of Radiology, West China Hospital, Sichuan University, Chengdu, China.
Department of Ultrasound, West China Hospital, Sichuan University, Chengdu, China.
Front Oncol. 2021 Feb 26;11:643051. doi: 10.3389/fonc.2021.643051. eCollection 2021.
To determine whether additional systematic biopsy is necessary in all biopsy naïve patients with MRI visible lesions by taking PI-RADS score and prostate volume into consideration.
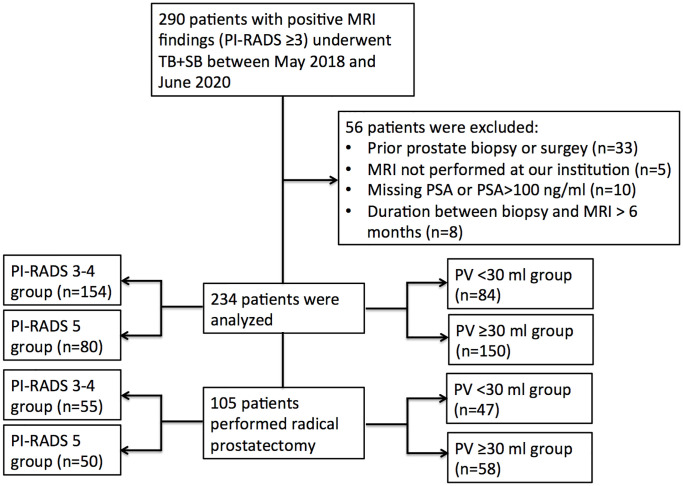
Patients who underwent combined systematic biopsy (SB) and cognitive MRI-targeted biopsy (TB) in our hospital between May 2018 and June 2020 were retrospectively reviewed. The detection rate of clinical significant prostate cancer (csPCa), biopsy grade group (GG) concordance, and disease upgrading rate on radical prostatectomy were compared between SB and TB and further stratified by PI-RADS v2.0 category and prostate volume.
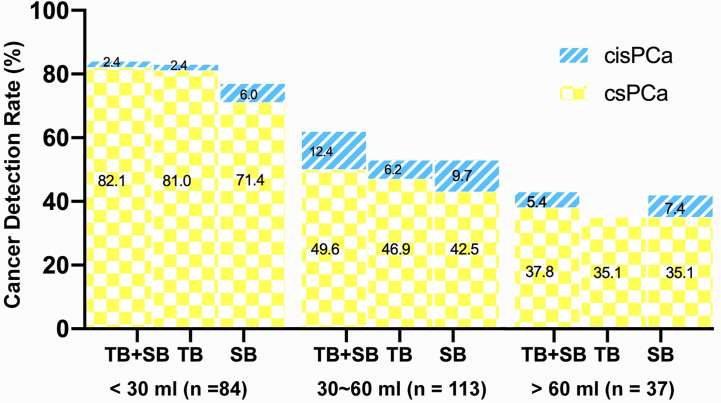
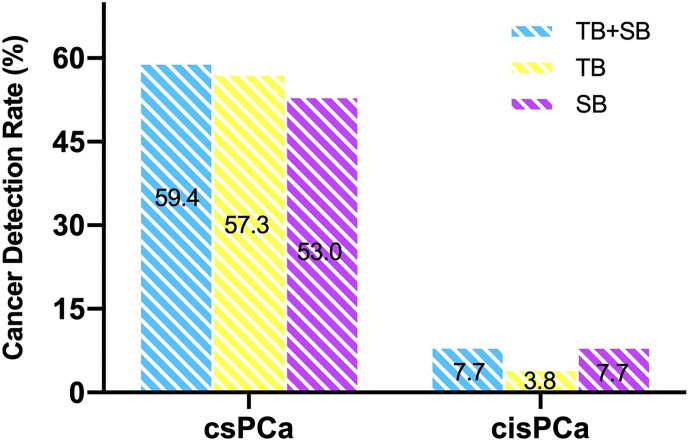
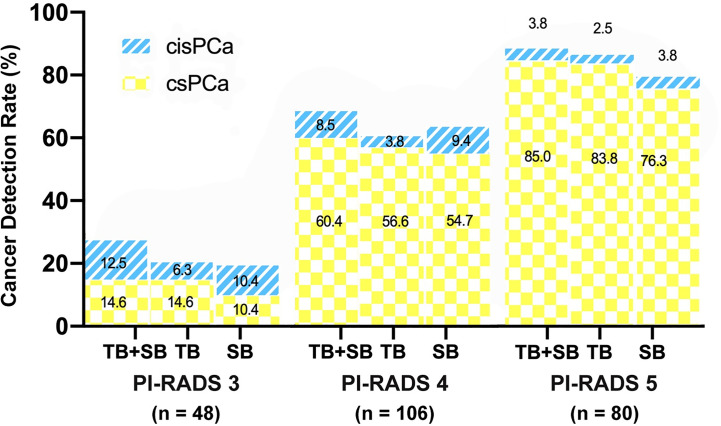
A total of 234 patients were analyzed in this study. TB alone detected more csPCa and less clinically insignificant prostate cancer (cisPCa) than SB alone in the whole cohort (57.3 53%, P = 0.041; 3.8 7.7%, P = 0.049 respectively). The additional SB indicated only a marginal increase of csPCa detection but a remarkable increase of cisPCa detection compared with targeted biopsy (59.4 57.3%, P = 0.064; 3.8 7.7%, P = 0.012). As stratified by PI-RADS category, the difference of csPCa detection rate between TB and SB was not significant either in PI-RADS 5 subgroup (83.8 76.3%, P = 0.07) or in PI-RADS 3-4 subgroup (43.5 40.9%, P = 1.0). Additional SB decreased the rate of disease upgrading on radical prostatectomy (RP) than TB alone in PI-RADS 3-4 subgroup (14.5 25.5%, P = 0.031) other than PI-RADS 5 subgroup (6 6%, P = 1.0). When stratified by prostate volume (PV), TB alone detected more csPCa than SB in small prostate (PV < 30 ml) group (81.0 71.0%, P = 0.021) but not in large prostate (PV ≥ 30 ml) group (44.0 42.7%, P = 0.754). The additional SB did not significantly decrease the rate of disease upgrading on RP than TB alone in either small or large prostate (6.4 8.5%, P = 1.0; 13.8 22.4%, P = 0.063).
The combination biopsy method was no superior than targeted biopsy alone in PI-RADS 5 or in small volume prostate subgroup.
通过考虑前列腺影像报告和数据系统(PI-RADS)评分及前列腺体积,确定对于所有初次活检且MRI可见病变的患者,是否有必要进行额外的系统活检。
回顾性分析2018年5月至2020年6月期间在我院接受联合系统活检(SB)和认知MRI靶向活检(TB)的患者。比较SB和TB之间临床显著前列腺癌(csPCa)的检出率、活检分级组(GG)一致性以及根治性前列腺切除术中疾病升级率,并进一步按PI-RADS v2.0类别和前列腺体积进行分层。
本研究共分析了234例患者。在整个队列中,单独TB检测出的csPCa比单独SB更多,而临床意义不显著的前列腺癌(cisPCa)更少(分别为57.3%对53%,P = 0.041;3.8%对7.7%,P = 0.049)。与靶向活检相比,额外的SB仅使csPCa检测略有增加,但cisPCa检测显著增加(59.4%对57.3%,P = 0.064;3.8%对7.7%,P = 0.012)。按PI-RADS类别分层,在PI-RADS 5亚组(83.8%对76.3%,P = 0.07)或PI-RADS 3 - 4亚组(43.5%对40.9%,P = 1.0)中,TB和SB之间csPCa检出率的差异均不显著。在PI-RADS 3 - 4亚组中,额外的SB比单独TB降低了根治性前列腺切除术(RP)中疾病升级的发生率(14.5%对25.5%,P = 0.031),而在PI-RADS 5亚组中无差异(6%对6%,P = 1.0)。按前列腺体积(PV)分层时,在小前列腺(PV < 30 ml)组中,单独TB检测出的csPCa比SB更多(81.0%对71.0%,P = 0.021),但在大前列腺(PV≥30 ml)组中无差异(44.0%对42.7%,P = 0.754)。在小前列腺或大前列腺组中,额外的SB与单独TB相比,在RP中疾病升级率的降低均不显著(6.4%对8.5%,P = 1.0;13.8%对22.4%,P = 0.063)。
在PI-RADS 5或小体积前列腺亚组中,联合活检方法并不优于单独的靶向活检。