Wenzel Mike, Welte Maria N, Grossmann Lina, Preisser Felix, Theissen Lena H, Humke Clara, Deuker Marina, Bernatz Simon, Gild Philipp, Ahyai Sascha, Karakiewicz Pierre I, Bodelle Boris, Kluth Luis A, Chun Felix K H, Mandel Philipp, Becker Andreas
Department of Urology, University Hospital Frankfurt, Goethe University Frankfurt am Main, Frankfurt, Germany.
Cancer Prognostics and Health Outcomes Unit, Division of Urology, University of Montréal Health Center, Montréal, QC, Canada.
Front Surg. 2021 Feb 25;8:633196. doi: 10.3389/fsurg.2021.633196. eCollection 2021.
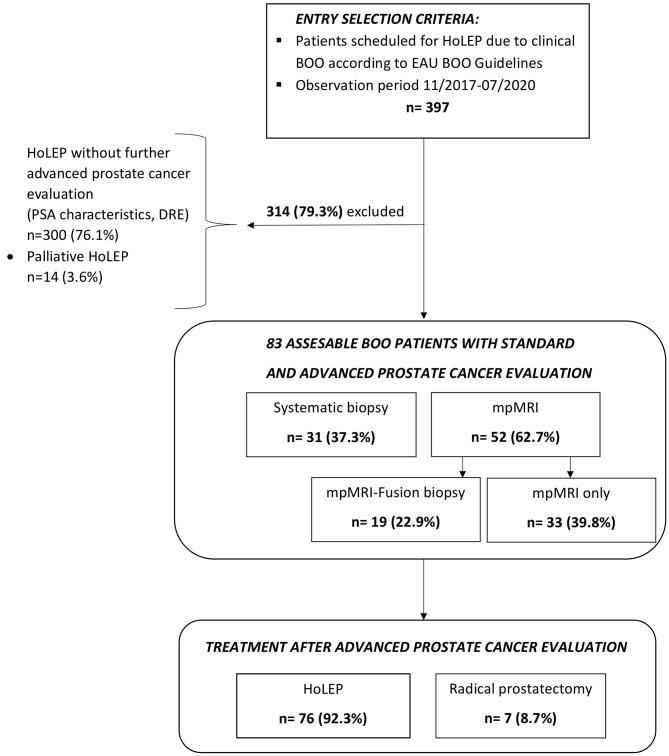
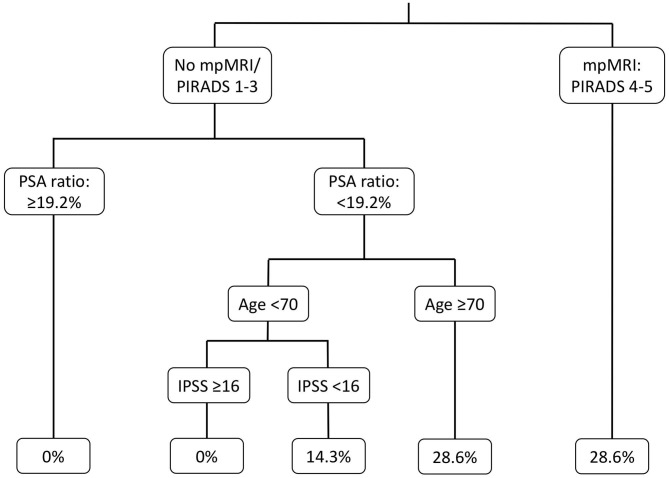
To investigate the value of standard [digital rectal examination (DRE), PSA] and advanced (mpMRI, prostate biopsy) clinical evaluation for prostate cancer (PCa) detection in contemporary patients with clinical bladder outlet obstruction (BOO) scheduled for Holmium laser enucleation of the prostate (HoLEP). We retrospectively analyzed 397 patients, who were referred to our tertiary care laser center for HoLEP due to BOO between 11/2017 and 07/2020. Of those, 83 (20.7%) underwent further advanced clinical PCa evaluation with mpMRI and/or prostate biopsy due to elevated PSA and/or lowered PSA ratio and/or suspicious DRE. Logistic regression and binary regression tree models were applied to identify PCa in BOO patients. An mpMRI was conducted in 56 (66%) of 83 patients and revealed PIRADS 4/5 lesions in 14 (25%) patients. Subsequently, a combined systematic randomized and MRI-fusion biopsy was performed in 19 (23%) patients and revealed in PCa detection in four patients (5%). A randomized prostate biopsy was performed in 31 (37%) patients and revealed in PCa detection in three patients (4%). All seven patients (9%) with PCa detection underwent radical prostatectomy with 29% exhibiting non-organ confined disease. Incidental PCa after HoLEP ( = 76) was found in nine patients (12%) with advanced clinical PCa evaluation preoperatively. In univariable logistic regression analyses, PSA, fPSA ratio, and PSA density failed to identify patients with PCa detection. Conversely, patients with a lower International Prostate Symptom Score (IPSS) and PIRADs 4/5 lesion in mpMRI were at higher risk for PCa detection. In multivariable adjusted analyses, PIRADS 4/5 lesions were confirmed as an independent risk factor (OR 9.91, = 0.04), while IPSS did not reach significance ( = 0.052). In advanced clinical PCa evaluation mpMRI should be considered in patients with elevated total PSA or low fPSA ratio scheduled for BOO treatment with HoLEP. Patients with low IPSS or PIRADS 4/5 lesions in mpMRI are at highest risk for PCa detection. In patients with a history of two or more sets of negative prostate biopsies, advanced clinical PCa evaluation might be omitted.
为了研究标准(直肠指检、前列腺特异性抗原)和高级(多参数磁共振成像、前列腺活检)临床评估对当代计划接受钬激光前列腺剜除术(HoLEP)治疗的临床膀胱出口梗阻(BOO)患者检测前列腺癌(PCa)的价值。我们回顾性分析了397例患者,这些患者在2017年11月至2020年7月期间因BOO被转诊至我们的三级医疗激光中心接受HoLEP治疗。其中,83例(20.7%)因前列腺特异性抗原升高和/或前列腺特异性抗原比值降低和/或直肠指检可疑而接受了进一步的高级临床PCa评估,包括多参数磁共振成像和/或前列腺活检。应用逻辑回归和二元回归树模型来识别BOO患者中的PCa。83例患者中有56例(66%)进行了多参数磁共振成像,其中14例(25%)显示前列腺影像报告和数据系统(PIRADS)4/5级病变。随后,19例(23%)患者进行了联合系统随机和磁共振融合活检,4例(5%)患者检测出PCa。31例(37%)患者进行了随机前列腺活检,3例(4%)患者检测出PCa。所有7例(9%)检测出PCa的患者均接受了根治性前列腺切除术,其中29%表现为非器官局限性疾病。术前进行高级临床PCa评估的患者中,9例(12%)在HoLEP术后发现了偶发PCa(n = 76)。在单变量逻辑回归分析中,前列腺特异性抗原、游离前列腺特异性抗原比值和前列腺特异性抗原密度未能识别出检测出PCa的患者。相反,国际前列腺症状评分较低且多参数磁共振成像中PIRADs 4/5级病变的患者检测出PCa的风险较高。在多变量调整分析中,PIRADS 4/5级病变被确认为独立危险因素(比值比9.91,P = 0.04),而国际前列腺症状评分未达到显著水平(P = 0.052)。对于计划接受HoLEP治疗BOO且总前列腺特异性抗原升高或游离前列腺特异性抗原比值低的患者,在高级临床PCa评估中应考虑多参数磁共振成像。国际前列腺症状评分低或多参数磁共振成像中PIRADS 4/5级病变的患者检测出PCa的风险最高。对于有两组或更多组前列腺活检阴性史的患者,可能无需进行高级临床PCa评估。