Ito Hiromasa, Masuda Jun, Kurita Tairo, Ida Mizuki, Yamamoto Ayato, Takasaki Akihiro, Takeuchi Tetsushiro, Sato Yuichi, Omura Takashi, Sawai Toshiki, Tanigawa Takashi, Ito Masaaki, Dohi Kaoru
Department of Cardiology and Nephrology, Mie University Graduate School of Medicine, Tsu, Japan.
Department of Cardiology, Mie Prefectural General Medical Center, Yokkaichi, Japan.
Int J Cardiol Heart Vasc. 2021 Feb 26;33:100738. doi: 10.1016/j.ijcha.2021.100738. eCollection 2021 Apr.
Chronic total occlusion (CTO) in a non-infarct-related artery (IRA) in patients with acute coronary syndrome (ACS) is associated with a poor prognosis. However, whether the prognostic impact of non-IRA CTO differs according to left ventricular ejection fraction (LVEF) is unclear.
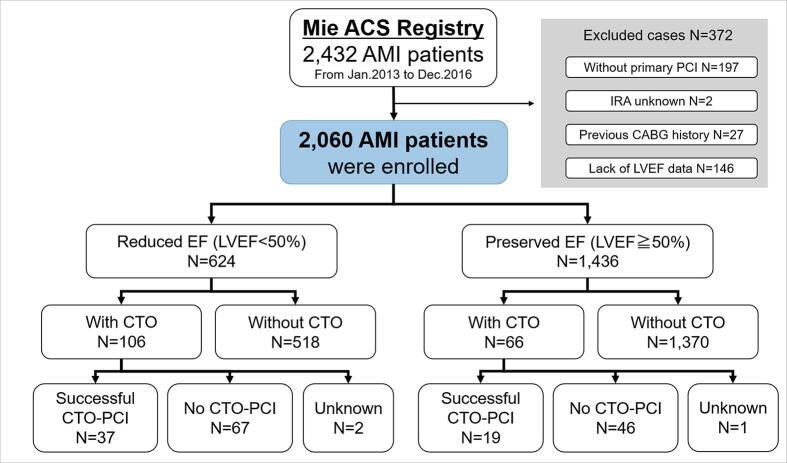
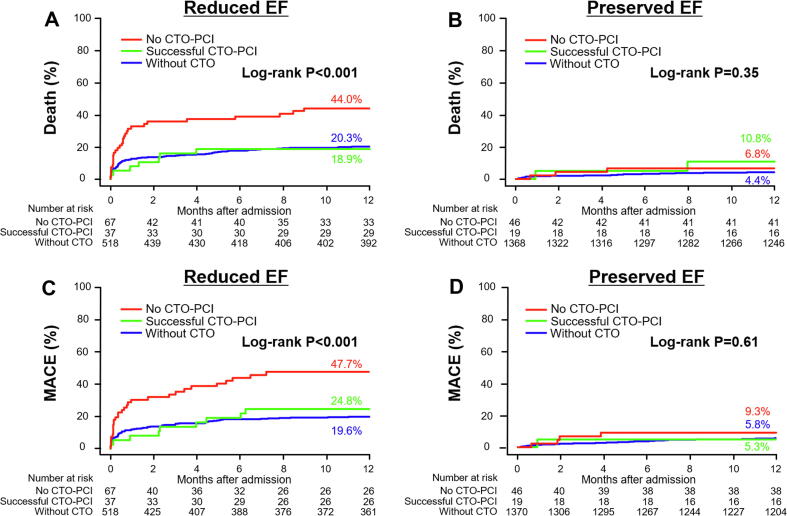
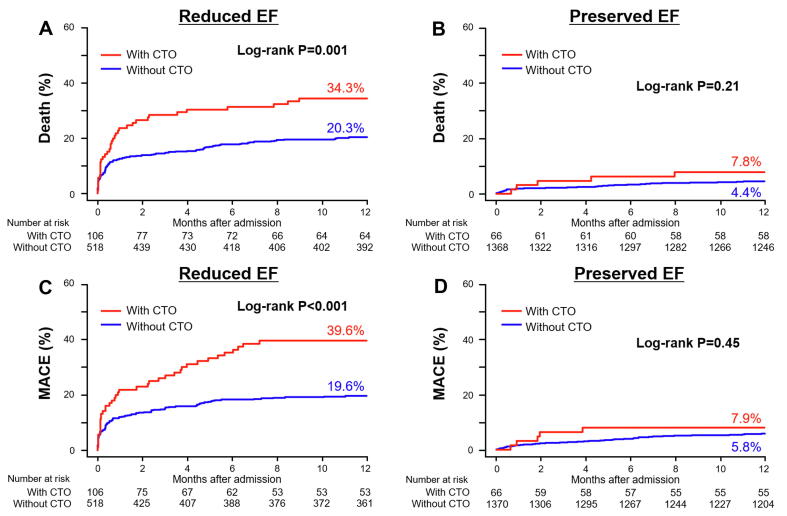
A total of 2060 consecutive acute myocardial infarction (AMI) patients who underwent primary percutaneous coronary intervention (PCI) were classified into 2 groups according to their LVEF (reduced EF: LVEF < 50%, preserved EF: LVEF ≥ 50%) and further subdivided according to the presence of concomitant non-IRA CTO. In the reduced EF group, patients with CTO had a higher 1-year all-cause death rate (20.3% vs. 34.3%, P = 0.001) and major adverse cardiac event rate (MACE: 19.6% vs. 39.6%, P < 0.001) compared to those without CTO, but they were similar between patients with and without CTO in the preserved EF group. Non-IRA CTO was an independent predictor of all-cause death (HR 1.58, 95% CI 1.06-2.33, P = 0.02) and MACE (HR 1.67, 95% CI 1.14-2.46, P = 0.009) only in the reduced EF group. In addition, the outcomes of successful CTO-PCI seemed to be similar to those without CTO in the reduced EF group.
CTO in a non-IRA may contribute to a poor prognosis only in AMI patients with reduced LVEF.
急性冠状动脉综合征(ACS)患者非梗死相关动脉(IRA)中的慢性完全闭塞(CTO)与预后不良相关。然而,非IRA CTO对预后的影响是否因左心室射血分数(LVEF)而异尚不清楚。
共有2060例接受直接经皮冠状动脉介入治疗(PCI)的急性心肌梗死(AMI)患者根据其LVEF分为两组(射血分数降低组:LVEF<50%,射血分数保留组:LVEF≥50%),并根据是否存在伴随的非IRA CTO进一步细分。在射血分数降低组中,与无CTO的患者相比,CTO患者的1年全因死亡率更高(20.3%对34.3%,P=0.001)和主要不良心脏事件发生率更高(MACE:19.6%对39.6%,P<0.001),但在射血分数保留组中,有CTO和无CTO的患者之间相似。仅在射血分数降低组中,非IRA CTO是全因死亡(HR 1.58,95%CI 1.06-2.33,P=0.02)和MACE(HR 1.67,95%CI 1.14-2.46,P=0.009)的独立预测因素。此外,在射血分数降低组中,成功的CTO-PCI结果似乎与无CTO的结果相似。
非IRA中的CTO可能仅在LVEF降低的AMI患者中导致预后不良。