Department of Pathology, Stanford University School of Medicine, Stanford, CA, USA.
Special Chemistry Laboratory, Stanford Healthcare, Palo Alto, CA, USA.
Clin Chem. 2021 Jul 6;67(7):977-986. doi: 10.1093/clinchem/hvab045.
Laboratory-based methods for SARS-CoV-2 antibody detection vary widely in performance. However, there are limited prospectively-collected data on assay performance, and minimal clinical information to guide interpretation of discrepant results.
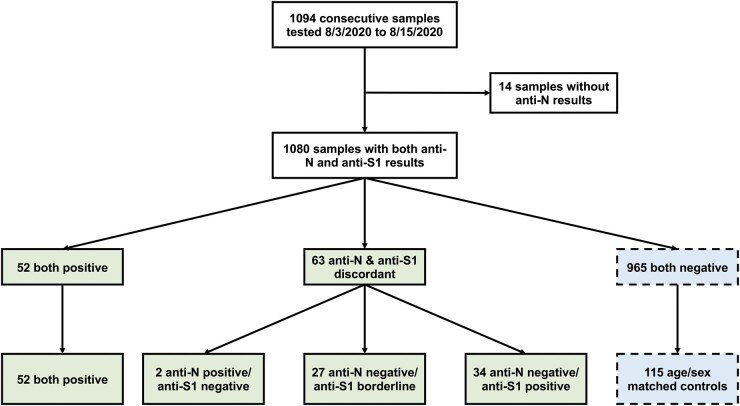
Over a 2-week period, 1080 consecutive plasma samples submitted for clinical SARS-CoV-2 IgG testing were tested in parallel for anti-nucleocapsid IgG (anti-N, Abbott) and anti-spike IgG (anti-S1, EUROIMMUN). Chart review was conducted for samples testing positive or borderline on either assay, and for an age/sex-matched cohort of samples negative by both assays. CDC surveillance case definitions were used to determine clinical sensitivity/specificity and conduct receiver operating characteristics curve analysis.
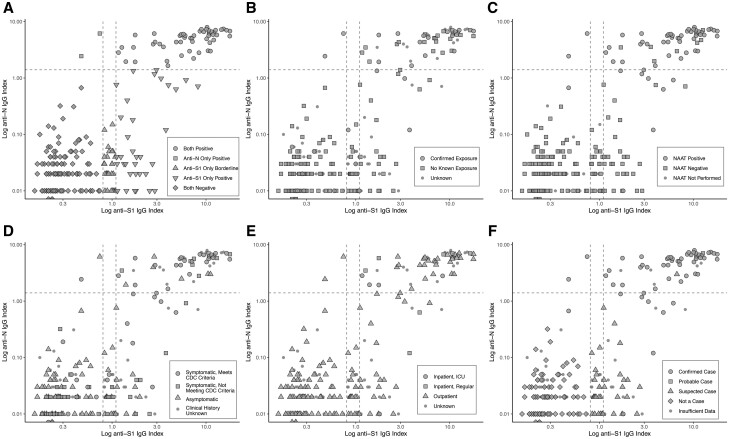
There were 52 samples positive by both methods, 2 positive for anti-N only, 34 positive for anti-S1 only, and 27 borderline for anti-S1. Of the 34 individuals positive for anti-S1 alone, 8 (24%) had confirmed COVID-19. No anti-S1 borderline cases were positive for anti-N or had confirmed/probable COVID-19. The anti-N assay was less sensitive (84.2% [95% CI 72.1-92.5%] vs 94.7% [95% CI 85.4-98.9%]) but more specific (99.2% [95% CI 95.5-100%] vs 86.9% [95% CI 79.6-92.3%]) than anti-S1. Abbott anti-N sensitivity could be improved to 96.5% with minimal effect on specificity if the index threshold was lowered from 1.4 to 0.6.
Real-world concordance between different serologic assays may be lower than previously described in retrospective studies. These findings have implications for the interpretation of SARS-CoV-2 IgG results, especially with the advent of spike antigen-targeted vaccination, as a subset of patients with true infection are anti-N negative and anti-S1 positive.
基于实验室的 SARS-CoV-2 抗体检测方法在性能上差异很大。然而,关于检测性能的前瞻性数据有限,并且很少有临床信息可以指导对不一致结果的解释。
在两周的时间内,对 1080 份连续提交用于临床 SARS-CoV-2 IgG 检测的血浆样本进行了平行检测,检测抗核衣壳 IgG(抗-N,雅培)和抗刺突 IgG(抗-S1,EUROIMMUN)。对两种检测方法均为阳性或临界值的样本以及两种检测方法均为阴性的年龄/性别匹配样本进行了图表审查。使用 CDC 监测病例定义来确定临床敏感性/特异性并进行接收者操作特征曲线分析。
有 52 份样本两种方法均为阳性,2 份仅抗-N 阳性,34 份仅抗-S1 阳性,27 份抗-S1 临界值。在仅抗-S1 阳性的 34 人中,有 8 人(24%)患有确诊的 COVID-19。没有抗-S1 临界值病例抗-N 阳性或患有确诊/可能的 COVID-19。抗-N 检测的敏感性较低(84.2%[95%CI72.1-92.5%] 与 94.7%[95%CI85.4-98.9%]),但特异性较高(99.2%[95%CI95.5-100%] 与 86.9%[95%CI79.6-92.3%])。如果将雅培抗-N 的指数阈值从 1.4 降低到 0.6,则可以将敏感性提高到 96.5%,而特异性的影响最小。
不同血清学检测方法之间的实际一致性可能低于回顾性研究中描述的。这些发现对 SARS-CoV-2 IgG 结果的解释有影响,特别是随着针对刺突抗原的疫苗接种的出现,因为一组真正感染的患者抗-N 阴性而抗-S1 阳性。