Department of Medicine, Division of Pulmonary and Critical Care, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA.
Université de Nantes, Centre Hospitalier Universitaire de Nantes, EA3826 Thérapeutiques Anti-Infectieuses, Service d'Anesthésie Réanimation Chirurgicale, Hôtel Dieu, Nantes, F-44000.
Clin Infect Dis. 2021 Aug 2;73(3):e710-e718. doi: 10.1093/cid/ciab032.
Hospital-acquired bacterial pneumonia (HABP) and ventilator-associated bacterial pneumonia (VABP) are associated with high mortality rates. We evaluated the efficacy and safety of tedizolid (administered as tedizolid phosphate) for treatment of gram-positive ventilated HABP/VABP.
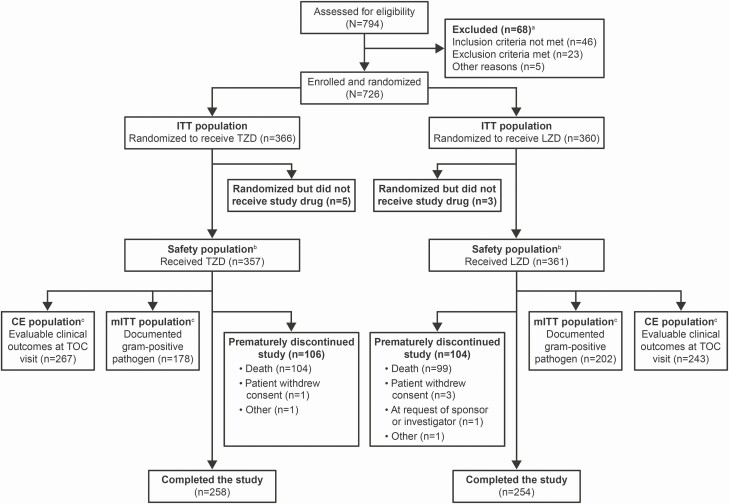
In this randomized, noninferiority, double-blind, double-dummy, global phase 3 trial, patients were randomized 1:1 to receive intravenous tedizolid phosphate 200 mg once daily for 7 days or intravenous linezolid 600 mg every 12 hours for 10 days. Treatment was 14 days in patients with concurrent gram-positive bacteremia. The primary efficacy end points were day 28 all-cause mortality (ACM; noninferiority margin, 10%) and investigator-assessed clinical response at test of cure (TOC; noninferiority margin, 12.5%) in the intention-to-treat population.
Overall, 726 patients were randomized (tedizolid, n = 366; linezolid, n = 360). Baseline characteristics, including incidence of methicillin-resistant Staphylococcus aureus (31.3% overall), were well balanced. Tedizolid was noninferior to linezolid for day 28 ACM rate: 28.1% and 26.4%, respectively (difference, -1.8%; 95% confidence interval [CI]: -8.2 to 4.7). Noninferiority of tedizolid was not demonstrated for investigator-assessed clinical cure at TOC (tedizolid, 56.3% vs linezolid, 63.9%; difference, -7.6%; 97.5% CI: -15.7 to 0.5). In post hoc analyses, no single factor accounted for the difference in clinical response between treatment groups. Drug-related adverse events occurred in 8.1% and 11.9% of patients who received tedizolid and linezolid, respectively.
Tedizolid was noninferior to linezolid for day 28 ACM in the treatment of gram-positive ventilated HABP/VABP. Noninferiority of tedizolid for investigator-assessed clinical response at TOC was not demonstrated. Both drugs were well tolerated.
NCT02019420.
医院获得性细菌性肺炎(HABP)和呼吸机相关性细菌性肺炎(VABP)与高死亡率相关。我们评估了替加环素(磷酸替加环素)治疗革兰阳性菌呼吸机相关性 HABP/VABP 的疗效和安全性。
在这项随机、非劣效性、双盲、双模拟、全球性 3 期试验中,患者按 1:1 随机接受静脉注射替加环素磷酸酯 200mg 每日 1 次治疗 7 天,或静脉注射利奈唑胺 600mg 每 12 小时 1 次治疗 10 天。对于合并革兰阳性菌菌血症的患者,治疗时间为 14 天。主要疗效终点为第 28 天全因死亡率(ACM;非劣效性边界为 10%)和治疗后评估的临床应答(TOC;非劣效性边界为 12.5%),在意向治疗人群中进行评估。
总体而言,726 名患者被随机分配(替加环素组,n=366;利奈唑胺组,n=360)。基线特征,包括耐甲氧西林金黄色葡萄球菌(总体 31.3%)的发生率,均平衡良好。替加环素治疗第 28 天的 ACM 率与利奈唑胺非劣效:分别为 28.1%和 26.4%(差异,-1.8%;95%置信区间[CI]:-8.2 至 4.7)。替加环素在 TOC 时的临床治愈率评估中未显示非劣效性:替加环素组为 56.3%,利奈唑胺组为 63.9%(差异,-7.6%;97.5%CI:-15.7 至 0.5)。事后分析中,没有单一因素可以解释治疗组之间临床反应的差异。接受替加环素和利奈唑胺治疗的患者中,分别有 8.1%和 11.9%发生药物相关不良事件。
替加环素治疗革兰阳性菌呼吸机相关性 HABP/VABP 的第 28 天 ACM 非劣效于利奈唑胺。替加环素在 TOC 时的临床反应评估中未显示非劣效性。两种药物均耐受良好。
NCT02019420。