Consultant, Department of Maternal, Newborn, Child and Adolescent Health, World Health Organization, Geneva, Switzerland.
Department of Community Health, Kinshasa School of Public Health, Kinshasa, Democratic Republic of Congo.
PLoS One. 2021 Mar 15;16(3):e0247977. doi: 10.1371/journal.pone.0247977. eCollection 2021.
Serious bacterial neonatal infections are a major cause of global neonatal mortality. While hospitalized treatment is recommended, families cannot access inpatient treatment in low resource settings. Two parallel randomized control trials were conducted at five sites in three countries (Democratic Republic of Congo, Kenya, and Nigeria) to compare the effectiveness of treatment with experimental regimens requiring fewer injections with a reference regimen A (injection gentamicin plus injection procaine penicillin both once daily for 7 days) on the outpatient basis provided to young infants (0-59 days) with signs of possible serious bacterial infection (PSBI) when the referral was not feasible. Costs were estimated to quantify the financial implications of scaleup, and cost-effectiveness of these regimens.
Direct economic costs (including personnel, drugs and consumable costs) were estimated for identification, prenatal and postnatal visits, assessment, classification, treatment and follow-up. Data on time spent by providers on each activity was collected from 83% of providers. Indirect marginal financial costs were estimated for non-consumables/capital, training, transport, communication, administration and supervision by considering only a share of the total research and health system costs considered important for the program. Total economic costs (direct plus indirect) per young infant treated were estimated based on 39% of young infants enrolled in the trial during 2012 and the number of days each treated during one year. The incremental cost-effectiveness ratio was calculated using treatment failure after one week as the outcome indicator. Experimental regimens were compared to the reference regimen and pairwise comparisons were also made.
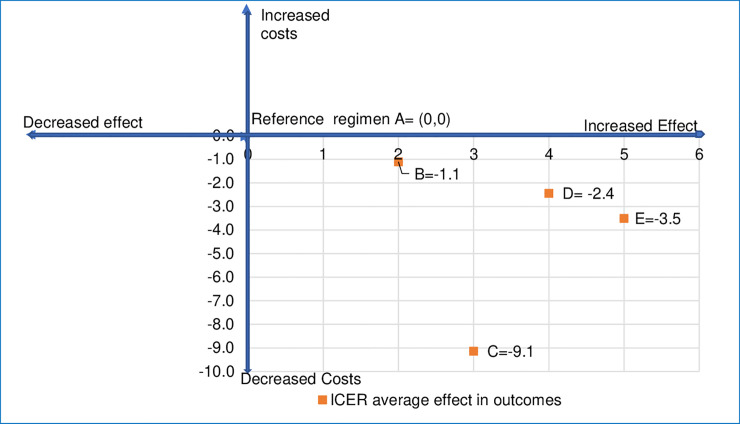
The average costs of treating a young infant with clinical severe infection (a sub-category of PSBI) in 2012 was lowest with regimen D (injection gentamicin once daily for 2 days plus oral amoxicillin twice daily for 7 days) at US$ 20.9 (95% CI US$ 16.4-25.3) or US$ 32.5 (2018 prices). While all experimental regimens B (injection gentamicin once daily plus oral amoxicillin twice daily, both for 7 days), regimen C (once daily of injection gentamicin injection plus injection procaine penicillin for 2 days, thereafter oral amoxicillin twice daily for 5 days) and regimen D were found to be more cost-effective as compared with the reference regimen A; pairwise comparison showed regimen D was more cost-effective than B or C. For fast breathing, the average cost of treatment with regimen E (oral amoxicillin twice daily for 7 days) at US$ 18.3 (95% CI US$ 13.4-23.3) or US$ 29.0 (2018 prices) was more cost-effective than regimen A. Indirect costs were 32% of the total treatment costs.
Scaling up of outpatient treatment for PSBI when the referral is not feasible with fewer injections and oral antibiotics is cost-effective for young infants and can lead to increased access to treatment resulting in potential reductions in neonatal mortality.
The trial was registered with Australian New Zealand Clinical Trials Registry under ID ACTRN 12610000286044.
严重的新生儿细菌感染是全球新生儿死亡的主要原因。虽然推荐住院治疗,但在资源匮乏的环境中,家庭无法获得住院治疗。在三个国家(刚果民主共和国、肯尼亚和尼日利亚)的五个地点进行了两项平行的随机对照试验,以比较在门诊基础上使用需要较少注射的实验方案(每天一次注射庆大霉素加注射普鲁卡因青霉素,共 7 天)与参考方案 A(每天一次注射庆大霉素加注射普鲁卡因青霉素,共 7 天)对有疑似严重细菌感染(PSBI)迹象的年轻婴儿(0-59 天)的治疗效果,当转诊不可行时。估计成本以量化扩大规模的财务影响,并评估这些方案的成本效益。
直接经济成本(包括人员、药品和消耗品成本)是根据识别、产前和产后访视、评估、分类、治疗和随访来估计的。从 83%的提供者那里收集了关于提供者在每项活动上花费的时间的数据。对于非消耗品/资本、培训、交通、通信、管理和监督的间接边际财务成本,仅考虑对该方案很重要的总研究和卫生系统成本的一部分进行了估计。根据 2012 年试验中登记的 39%的年轻婴儿和每个治疗的婴儿在一年内接受治疗的天数,估计了每个接受治疗的年轻婴儿的总经济成本(直接加间接)。使用一周后治疗失败作为结果指标计算增量成本效益比。将实验方案与参考方案进行比较,并进行两两比较。
2012 年,用方案 D(每天一次注射庆大霉素 2 天加口服阿莫西林 2 次,共 7 天)治疗有临床严重感染(PSBI 的一个亚类)的年轻婴儿的平均成本最低,为 20.9 美元(95%CI 16.4-25.3 美元)或 32.5 美元(2018 年价格)。虽然所有实验方案 B(每天一次注射庆大霉素加口服阿莫西林,均为 7 天)、方案 C(每天一次注射庆大霉素加注射普鲁卡因青霉素,共 2 天,此后口服阿莫西林,共 5 天)和方案 D 均被发现比参考方案 A 更具成本效益;但两两比较显示方案 D 比 B 或 C 更具成本效益。对于呼吸急促,用方案 E(每天口服阿莫西林 2 次,共 7 天)治疗的平均成本为 18.3 美元(95%CI 13.4-23.3 美元)或 29.0 美元(2018 年价格)比方案 A 更具成本效益。间接成本占总治疗成本的 32%。
对于转诊不可行的 PSBI 患者,采用较少注射和口服抗生素的门诊治疗是具有成本效益的,可以增加治疗机会,从而有可能降低新生儿死亡率。
该试验在澳大利亚和新西兰临床试验注册中心注册,编号为 ACTRN 12610000286044。