Department of Cardiology, University Hospital Dorset NHS Foundation Trust, Longfleet Rd., Poole, BH15 2JB, UK.
Department of Postgraduate Medical Education, Bournemouth University, Bournemouth, BH1 3LT, UK.
BMC Cardiovasc Disord. 2021 Mar 16;21(1):139. doi: 10.1186/s12872-021-01946-2.
The ambulatory arterial stiffness index (AASI) is an indirect measure of arterial stiffness obtained during ambulatory blood pressuring monitoring (ABPM). Its relationship to nocturnal blood pressure dipping status and major adverse cardiovascular events (MACE) are controversial and its association with vascular inflammation has not been examined. We aimed to investigate the relationship between the AASI, inflammation and nocturnal blood pressure dipping status and its association with MACE.
Adults (aged 18-80 years) who underwent 24-h ABPM for the diagnosis of hypertension or its control were included. The inflammatory markers measured were the neutrophil-lymphocyte (NLR), platelet-lymphocyte (PLR) and monocyte-lymphocyte ratios (MLR). The primary MACE was a composite of cardiovascular death, acute limb ischaemia, stroke or transient ischaemic attack (TIA) or acute coronary syndrome.
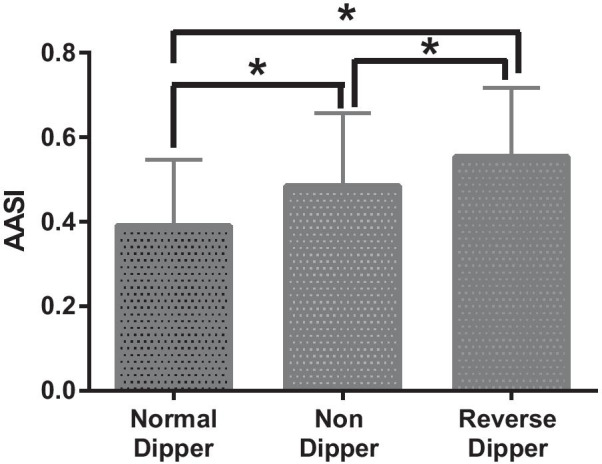
A total of 508 patients (51.2% female) aged 58.8 ± 14.0 years were included; 237 (46.7%) were normal-dippers (≥ 10% nocturnal systolic dip), 214 (42.1%) were non-dippers (0-10% dip) and 57 (11.2%) were reverse-dippers (< 0% dip). The AASI was significantly higher among reverse (0.56 ± 0.16) and non-dippers (0.48 ± 0.17) compared with normal dippers (0.39 ± 0.16; p < 0.0001) and correlated with the NLR (r = 0.20; 95% CI 0.11 to 0.29: < 0.0001) and systolic blood pressure dipping % (r = - 0.34; - 0.42 to - 0.26: p < 0.0001). Overall 39 (7.7%) patients had ≥ 1 MACE which included a total of seven cardiovascular deaths and 14 non-fatal strokes/TIAs. The mean follow up was 113.7 ± 64.0 weeks. Increasing NLR, but not AASI or systolic dipping, was independently linked to MACE (overall model Chi-square 60.67; p < 0.0001) and MLR to cardiovascular death or non-fatal stroke/TIA (overall model Chi-square 37.08; p < 0.0001).
In conclusion AASI was associated with blood pressure dipping and chronic inflammation but not independently to MACE. The MLR and NLR were independent predictors of MACE.
动态动脉僵硬度指数(AASI)是通过动态血压监测(ABPM)获得的动脉僵硬度的间接测量值。其与夜间血压下降状态和主要不良心血管事件(MACE)之间的关系存在争议,其与血管炎症的关系尚未被检测到。我们旨在研究 AASI、炎症与夜间血压下降状态之间的关系,并探讨其与 MACE 的相关性。
纳入了因高血压或其控制而行 24 小时 ABPM 的成年人(年龄 18-80 岁)。测量的炎症标志物为中性粒细胞-淋巴细胞(NLR)、血小板-淋巴细胞(PLR)和单核细胞-淋巴细胞比值(MLR)。主要 MACE 是心血管死亡、急性肢体缺血、卒中和短暂性脑缺血发作(TIA)或急性冠脉综合征的复合事件。
共纳入 508 例患者(51.2%为女性),年龄 58.8±14.0 岁;237 例(46.7%)为正常夜间血压下降者(夜间收缩压下降≥10%),214 例(42.1%)为非夜间血压下降者(夜间收缩压下降 0-10%),57 例(11.2%)为夜间血压反跳者(夜间收缩压下降<0%)。夜间血压反跳者(0.56±0.16)和夜间血压无下降者(0.48±0.17)的 AASI 明显高于正常夜间血压下降者(0.39±0.16;p<0.0001),且与 NLR(r=0.20;95%CI 0.11 至 0.29;<0.0001)和收缩压下降百分比(r=-0.34;-0.42 至-0.26;p<0.0001)呈正相关。总体上,有 39 例(7.7%)患者发生了≥1 次主要不良心血管事件,其中包括 7 例心血管死亡和 14 例非致命性卒中和 TIA。平均随访 113.7±64.0 周。NLR 增加(而不是 AASI 或收缩压下降)与 MACE 独立相关(总模型卡方值为 60.67;p<0.0001),MLR 与心血管死亡或非致命性卒中和 TIA 独立相关(总模型卡方值为 37.08;p<0.0001)。
AASI 与血压下降和慢性炎症相关,但与 MACE 不相关。MLR 和 NLR 是 MACE 的独立预测因子。