From the Department of Radiology (R.G., J.H.) and Julius Center for Health Sciences and Primary Care (R.G., M.I.G.), University Medical Center Utrecht and Utrecht University; and Department of Radiology (M.J.-C., J.d.B.), Leiden University Medical Center, the Netherlands.
Neurology. 2021 Apr 27;96(17):e2172-e2183. doi: 10.1212/WNL.0000000000011827. Epub 2021 Mar 16.
To determine whether white matter hyperintensity (WMH) markers on MRI are associated with long-term risk of mortality and ischemic stroke.
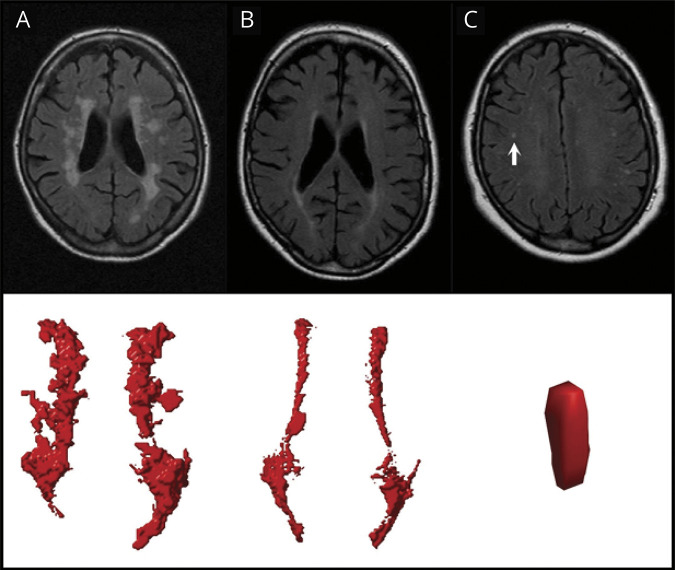
We included consecutive patients with manifest arterial disease enrolled in the Second Manifestations of Arterial Disease-Magnetic Resonance (SMART-MR) study. We obtained WMH markers (volume, type, and shape) from brain MRI scans performed at baseline using an automated algorithm. During follow-up, occurrence of death and ischemic stroke was recorded. Using Cox regression, we investigated associations of WMH markers with risk of mortality and ischemic stroke, adjusting for demographics, cardiovascular risk factors, and cerebrovascular disease.
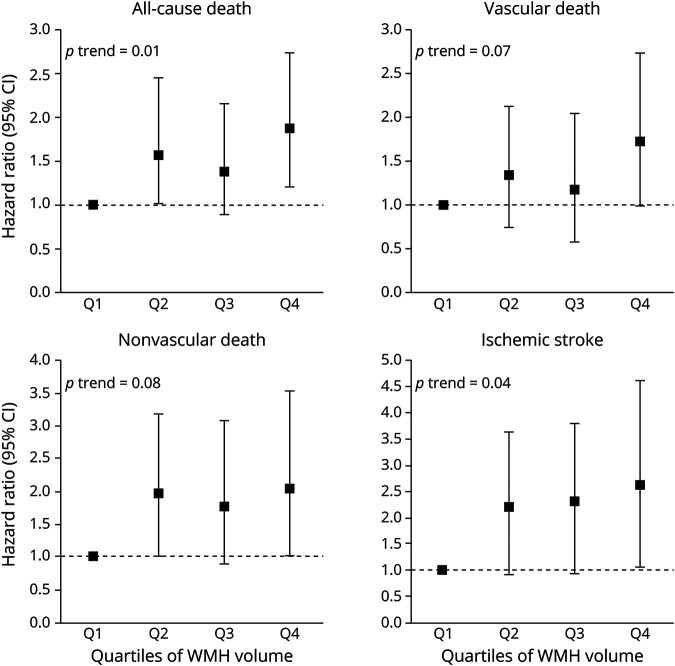
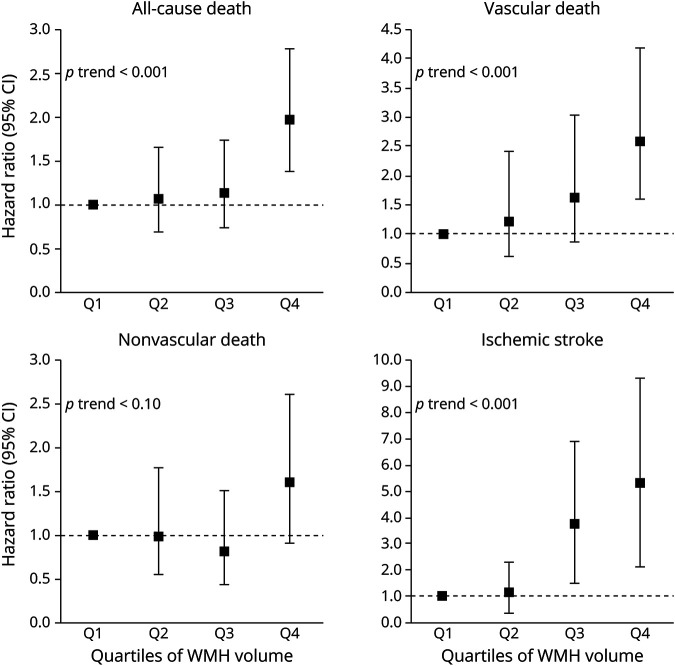
We included 999 patients (59 ± 10 years; 79% male) with a median follow-up of 12.5 years (range 0.2-16.0 years). A greater periventricular or confluent WMH volume was independently associated with a greater risk of vascular death (hazard ratio [HR] 1.29, 95% confidence interval [CI] 1.13-1.47) for a 1-unit increase in natural log-transformed WMH volume and ischemic stroke (HR 1.53, 95% CI 1.26-1.86). A confluent WMH type was independently associated with a greater risk of vascular (HR 1.89, 95% CI 1.15-3.11) and nonvascular death (HR 1.65, 95% CI 1.01-2.73) and ischemic stroke (HR 2.83, 95% CI 1.36-5.87). A more irregular shape of periventricular or confluent WMH, as expressed by an increase in concavity index, was independently associated with a greater risk of vascular (HR 1.20, 95% CI 1.05-1.38 per SD increase) and nonvascular death (HR 1.21, 95% CI 1.03-1.42) and ischemic stroke (HR 1.28, 95% CI 1.05-1.55).
WMH volume, type, and shape are associated with long-term risk of mortality and ischemic stroke in patients with manifest arterial disease.
确定磁共振成像上的脑白质高信号(WMH)标志物是否与长期死亡率和缺血性卒中风险相关。
我们纳入了连续入组的、表现性动脉疾病(Second Manifestations of Arterial Disease,SMART)研究中的磁共振成像(Magnetic Resonance,MR)患者。我们使用自动算法从基线脑 MRI 扫描中获得 WMH 标志物(体积、类型和形状)。在随访期间,记录死亡和缺血性卒中的发生情况。我们使用 Cox 回归分析,在校正人口统计学、心血管危险因素和脑血管疾病后,研究了 WMH 标志物与死亡率和缺血性卒中风险的相关性。
我们纳入了 999 例患者(59±10 岁,79%为男性),中位随访时间为 12.5 年(范围 0.2-16.0 年)。脑室周围或弥漫性 WMH 体积每增加 1 个单位,与血管性死亡(危险比 [hazard ratio,HR] 1.29,95%置信区间 [confidence interval,CI] 1.13-1.47)和缺血性卒中(HR 1.53,95%CI 1.26-1.86)风险的增加显著相关。弥漫性 WMH 类型与血管性(HR 1.89,95%CI 1.15-3.11)和非血管性(HR 1.65,95%CI 1.01-2.73)死亡以及缺血性卒中(HR 2.83,95%CI 1.36-5.87)风险的增加显著相关。脑室周围或弥漫性 WMH 形状不规则程度(用凹度指数增加表示)的增加与血管性(HR 1.20,95%CI 每增加 1 个标准差 [standard deviation,SD] 为 1.05-1.38)和非血管性(HR 1.21,95%CI 1.03-1.42)死亡和缺血性卒中(HR 1.28,95%CI 1.05-1.55)风险的增加显著相关。
在表现性动脉疾病患者中,WMH 体积、类型和形状与长期死亡率和缺血性卒中风险相关。