Department of Radiation Oncology, The Fourth Hospital of Hebei Medical University, Shijiazhuang, 050011, Hebei, China.
Department of General Surgery, The Fourth Hospital of Hebei Medical University, Shijiazhuang, 050011, Hebei, China.
BMC Surg. 2021 Mar 17;21(1):137. doi: 10.1186/s12893-021-01136-z.
To analyze whether neoadjuvant chemoradiotherapy (nCRT) could improve the survival for patients with adenocarcinoma of the esophagogastric junction compared with neoadjuvant chemotherapy (nCT). Both neoadjuvant chemotherapy alone and chemoradiotherapy before surgery have been shown to improve overall long-term survival for patients with adenocarcinoma in the esophagus or esophagogastric junction compared to surgery alone. It remains controversial whether nCRT is superior to nCT.
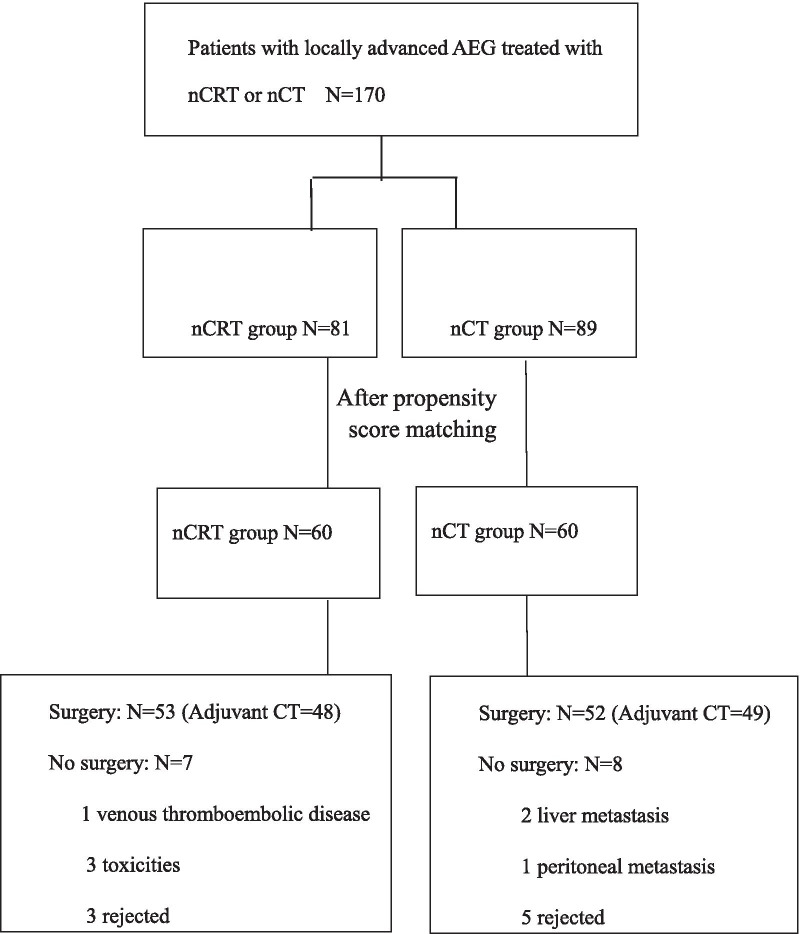
170 Patients with locally advanced (cT3-4NxM0) Siewert II and III adenocarcinoma of the esophagogastric junction (AEG) were treated with neoadjuvant chemotherapy consisting of capecitabine plus oxaliplatin with or without concurrent radiotherapy in the Fourth Hospital of Hebei Medical University. Intensity-modulated radiation therapy (IMRT) was used and delivered in 5 daily fractions of 1.8 Gy per week for 5 weeks (total dose of PTV: 45 Gy). 120 Patients were included in the propensity score matching (PSM) analysis to compare the effects of nCRT with nCT on survival.
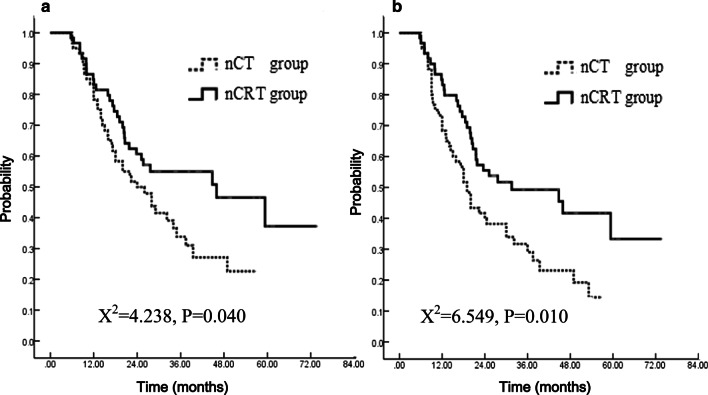
With a median follow-up of 41.2 months for patients alive after propensity score matching analysis, the 1- and 3-year OS were 84.8%, 55.0% in nCRT group and 78.3%, 38.3% in nCT group (P = 0.040; HR = 1.65, 95% CI 1.02-2.69). The 1- and 3-year PFS were 84.9%, 49.2% in nCRT group and 68.3%, 29.0% in nCT group (P = 0.010; HR = 1.80, 95% CI 1.14-2.85). The pathological complete response (pCR) was 17.0% in nCRT group and 1.9% in nCT group (P = 0.030). No significant difference was observed in postoperative complications between the two groups.
The nCRT confers a better survival with improved R0 resection rate and pCR rate compared with nCT for the patients with locally advanced AEG.
分析新辅助放化疗(nCRT)是否优于新辅助化疗(nCT),以改善食管胃结合部腺癌患者的生存。与单纯手术相比,新辅助化疗联合手术以及术前放化疗均可提高食管癌或食管胃结合部腺癌患者的总体长期生存率。nCRT 是否优于 nCT 仍存在争议。
170 例局部晚期(cT3-4NxM0)Siewert II 和 III 型食管胃结合部腺癌(AEG)患者在河北医科大学第四医院接受新辅助化疗,方案为卡培他滨联合奥沙利铂,联合或不联合同期放疗。采用调强放疗(IMRT),每周 5 次,每次 1.8 Gy,共 5 周(PTV 总剂量:45 Gy)。120 例患者纳入倾向评分匹配(PSM)分析,以比较 nCRT 与 nCT 对生存的影响。
对倾向性评分匹配分析后存活患者进行中位随访 41.2 个月,nCRT 组的 1 年和 3 年 OS 率分别为 84.8%和 55.0%,nCT 组分别为 78.3%和 38.3%(P=0.040;HR=1.65,95%CI 1.02-2.69)。nCRT 组的 1 年和 3 年 PFS 率分别为 84.9%和 49.2%,nCT 组分别为 68.3%和 29.0%(P=0.010;HR=1.80,95%CI 1.14-2.85)。nCRT 组的病理完全缓解(pCR)率为 17.0%,nCT 组为 1.9%(P=0.030)。两组术后并发症发生率无统计学差异。
与 nCT 相比,nCRT 可提高局部晚期 AEG 患者的 R0 切除率和 pCR 率,从而改善生存。