Topal Divan Gabriel, Aleksov Ahtarovski Kiril, Lønborg Jacob, Høfsten Dan, Nepper-Christensen Lars, Kyhl Kasper, Schoos Mikkel, Ghotbi Adam Ali, Göransson Christoffer, Bertelsen Litten, Holmvang Lene, Helqvist Steffen, Pedersen Frants, Schnabel Renate, Køber Lars, Kelbæk Henning, Vejlstrup Niels, Engstrøm Thomas, Clemmensen Peter
Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Denmark.
Department of Cardiology, University Heart Center Hamburg, Universitätsklinikum Hamburg-Eppendorf, Hamburg, Germany.
Int J Cardiol Heart Vasc. 2021 Mar 2;33:100731. doi: 10.1016/j.ijcha.2021.100731. eCollection 2021 Apr.
Coronary collateral circulation and conditioning from remote ischemic coronary territories may protect culprit myocardium in the elderly, and younger STEMI patients could suffer from larger infarcts. We evaluated the impact of age on myocardial salvage and long-term prognosis in a contemporary STEMI cohort.
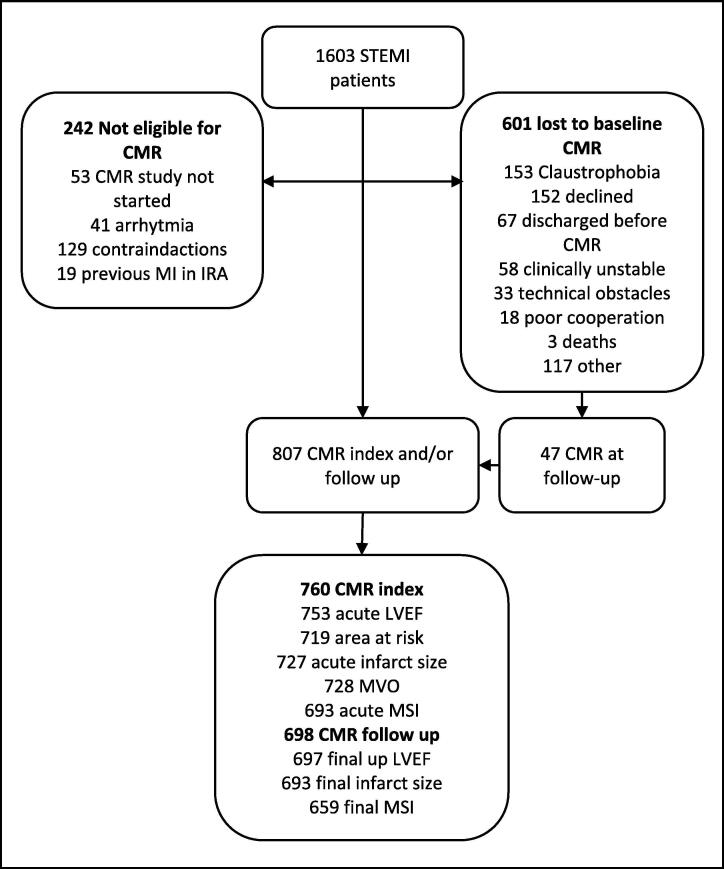
Of 1603 included STEMI patients 807 underwent cardiac magnetic resonance. To assess the impact of age on infarct size and left ventricular ejection fraction (LVEF) as well as the composite endpoint of death and re-hospitalization for heart failure we stratified the patients by an age cut-off of 60 years.
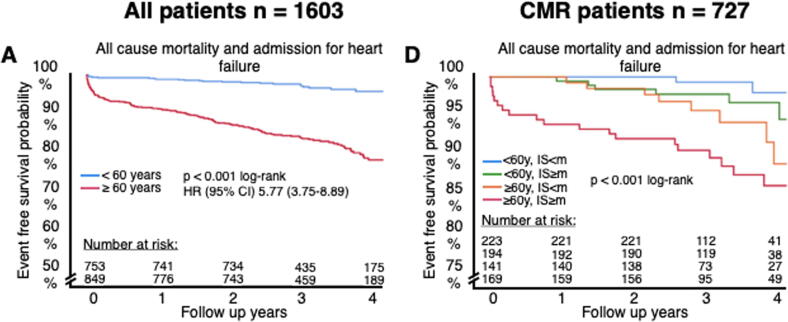
Younger STEMI patients had smaller final infarcts (10% vs. 12%, P = 0.012) and higher final LVEF (60% vs. 58%, P = 0.042). After adjusting for multiple potential confounders age did not remain significantly associated with infarct size and LVEF. During 4-year follow-up, the composite endpoint occurred less often in the young (3.2% vs. 17.2%; P < 0.001) with a univariate hazard ratio of 5.77 (95% CI, 3.75-8.89; p < 0.001). Event estimates of 4 subgroups (young vs. elderly and infarct size beyond vs. below median) showed a gradual increase in the occurrence of the composite endpoint depending on both age and acute infarct size (log-rank p < 0.001).
Having a STEMI after entering the seventh decade of life more than quadrupled the risk of future death or re-hospitalization for heart failure. Risk of death and re-hospitalization depended on both advanced age and infarct size, albeit no substantial difference was found in infarct size, LVEF and salvage potential between younger and elderly patients with STEMI.
冠状动脉侧支循环以及来自远程缺血性冠状动脉区域的预处理可能会保护老年患者的罪犯心肌,而年轻的ST段抬高型心肌梗死(STEMI)患者可能会发生更大面积的梗死。我们评估了年龄对当代STEMI队列中心肌挽救和长期预后的影响。
在纳入的1603例STEMI患者中,807例接受了心脏磁共振检查。为了评估年龄对梗死面积和左心室射血分数(LVEF)以及死亡和因心力衰竭再次住院的复合终点的影响,我们以60岁为年龄界限对患者进行分层。
年轻的STEMI患者最终梗死面积较小(10%对12%,P = 0.012),最终LVEF较高(60%对58%,P = 0.042)。在对多个潜在混杂因素进行调整后,年龄与梗死面积和LVEF不再显著相关。在4年的随访期间,年轻患者中复合终点的发生频率较低(3.2%对17.2%;P < 0.001),单因素风险比为5.77(95%CI,3.75 - 8.89;p < 0.001)。4个亚组(年轻与老年以及梗死面积高于与低于中位数)的事件估计显示,根据年龄和急性梗死面积,复合终点的发生率逐渐增加(对数秩检验p < 0.001)。
进入七十岁后发生STEMI会使未来死亡或因心力衰竭再次住院的风险增加四倍多。死亡和再次住院的风险取决于高龄和梗死面积,尽管在年轻和老年STEMI患者之间,梗死面积、LVEF和挽救潜力没有实质性差异。