Research Group in Perioperative Medicine, Hospital Universitario y Politécnico la Fe, Avinguda de Fernando Abril Martorell 106, 46026, Valencia, Spain.
Department of Anesthesiology, Hospital Universitario y Politécnico la Fe, Valencia, Spain.
BMC Anesthesiol. 2021 Mar 19;21(1):84. doi: 10.1186/s12871-021-01268-y.
It is uncertain whether the association of the intraoperative driving pressure (ΔP) with postoperative pulmonary complications (PPCs) depends on the surgical approach during abdominal surgery. Our primary objective was to determine and compare the association of time-weighted average ΔP (ΔP) with PPCs. We also tested the association of ΔP with intraoperative adverse events.
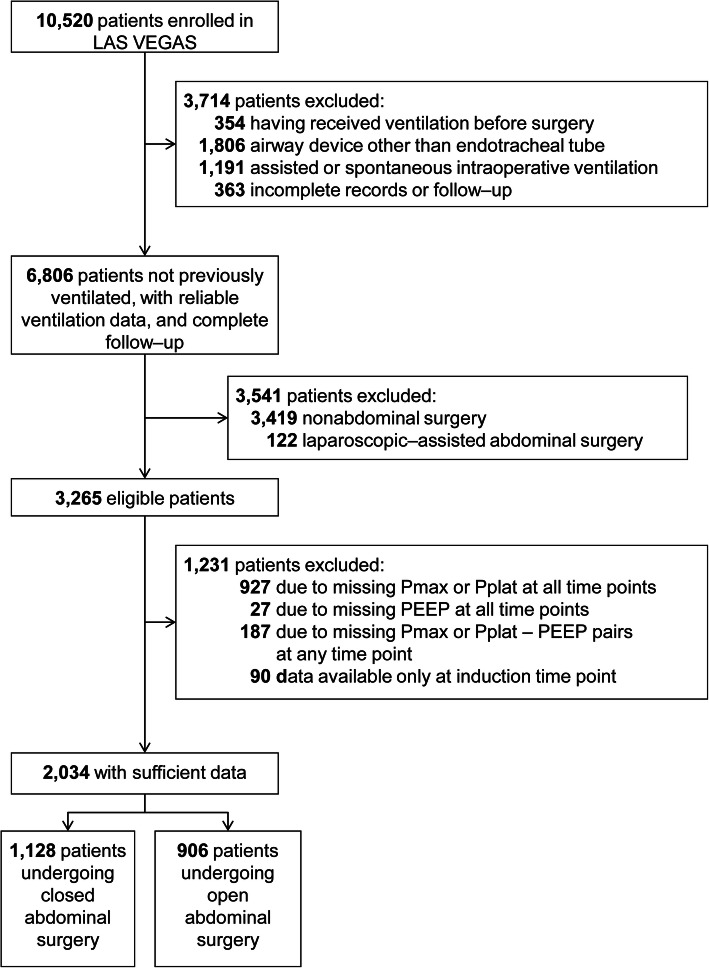
Posthoc retrospective propensity score-weighted cohort analysis of patients undergoing open or closed abdominal surgery in the 'Local ASsessment of Ventilatory management during General Anaesthesia for Surgery' (LAS VEGAS) study, that included patients in 146 hospitals across 29 countries. The primary endpoint was a composite of PPCs. The secondary endpoint was a composite of intraoperative adverse events.
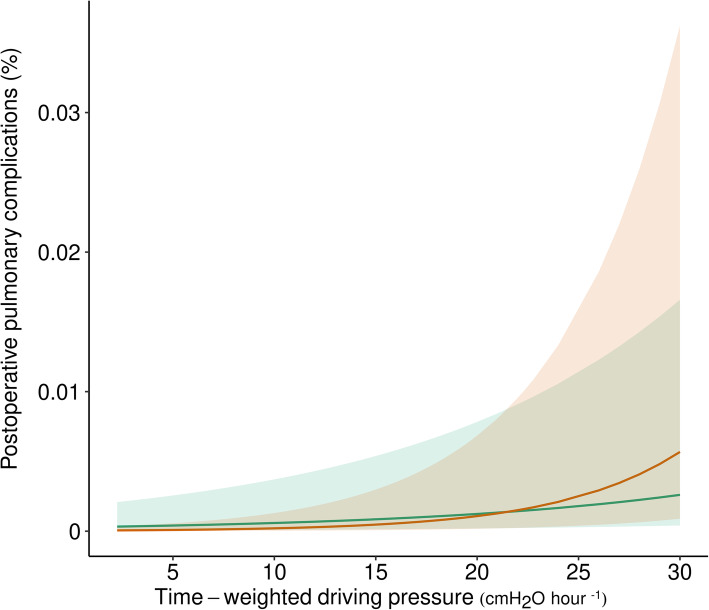
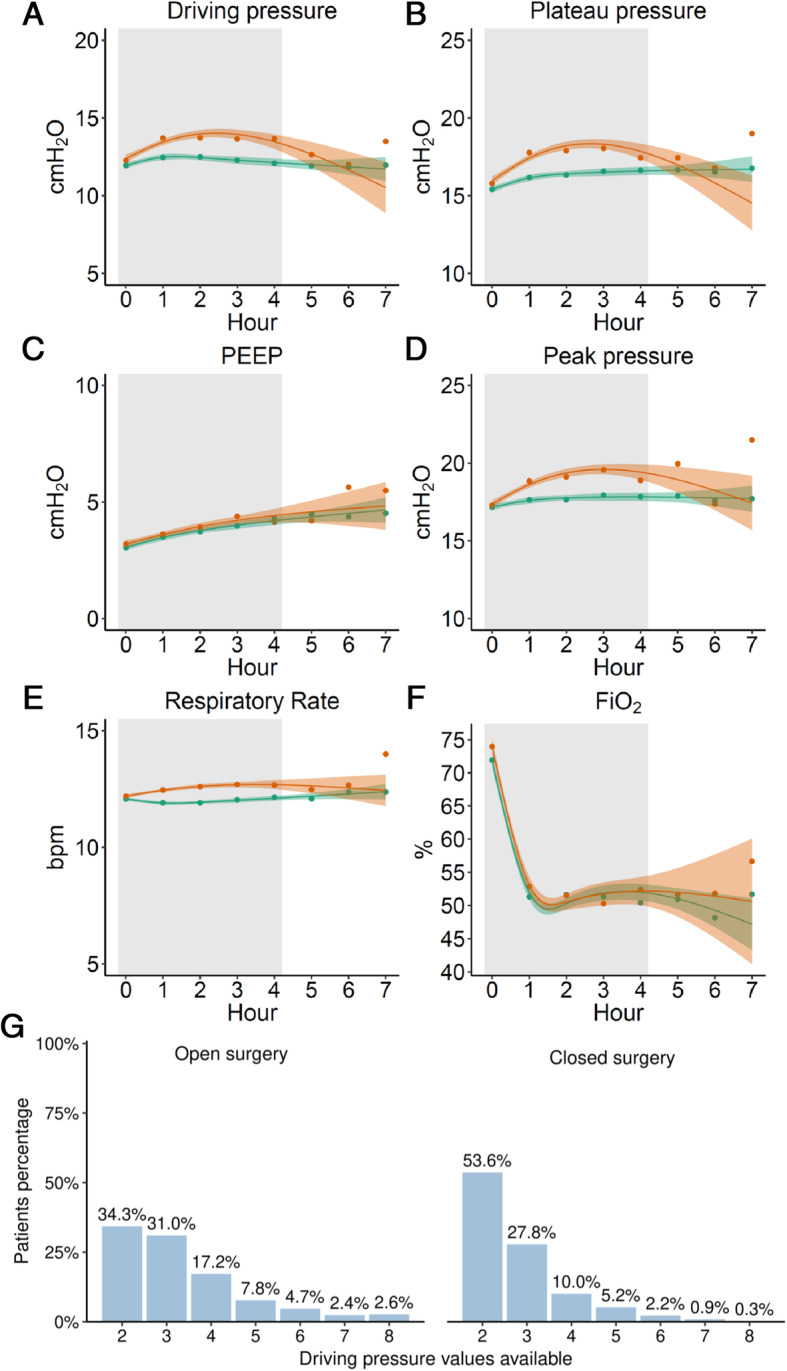
The analysis included 1128 and 906 patients undergoing open or closed abdominal surgery, respectively. The PPC rate was 5%. ΔP was lower in open abdominal surgery patients, but ΔP was not different between groups. The association of ΔP with PPCs was significant in both groups and had a higher risk ratio in closed compared to open abdominal surgery patients (1.11 [95%CI 1.10 to 1.20], P < 0.001 versus 1.05 [95%CI 1.05 to 1.05], P < 0.001; risk difference 0.05 [95%CI 0.04 to 0.06], P < 0.001). The association of ΔP with intraoperative adverse events was also significant in both groups but had higher odds ratio in closed compared to open abdominal surgery patients (1.13 [95%CI 1.12- to 1.14], P < 0.001 versus 1.07 [95%CI 1.05 to 1.10], P < 0.001; risk difference 0.05 [95%CI 0.030.07], P < 0.001).
ΔP is associated with PPC and intraoperative adverse events in abdominal surgery, both in open and closed abdominal surgery.
LAS VEGAS was registered at clinicaltrials.gov (trial identifier NCT01601223 ).
在腹部手术中,术中驱动压(ΔP)与术后肺部并发症(PPCs)的关联是否取决于手术入路尚不确定。我们的主要目的是确定并比较时间加权平均ΔP(ΔP)与 PPCs 的关联。我们还测试了ΔP 与术中不良事件的关联。
对接受开放或闭合腹部手术的患者进行事后回顾性倾向评分加权队列分析,该研究纳入了 29 个国家 146 家医院的患者。主要终点是 PPCs 的复合指标。次要终点是术中不良事件的复合指标。
分析纳入了分别接受开放或闭合腹部手术的 1128 例和 906 例患者。PPC 发生率为 5%。开放腹部手术患者的ΔP 较低,但两组之间的ΔP 无差异。ΔP 与 PPCs 的关联在两组中均有统计学意义,并且闭合组的风险比高于开放组(1.11 [95%CI 1.10 至 1.20],P<0.001 与 1.05 [95%CI 1.05 至 1.05],P<0.001;风险差异 0.05 [95%CI 0.04 至 0.06],P<0.001)。ΔP 与术中不良事件的关联在两组中均有统计学意义,但闭合组的优势比高于开放组(1.13 [95%CI 1.12 至 1.14],P<0.001 与 1.07 [95%CI 1.05 至 1.10],P<0.001;风险差异 0.05 [95%CI 0.03 至 0.07],P<0.001)。
ΔP 与腹部手术中的 PPC 和术中不良事件相关,无论是在开放还是闭合腹部手术中。
LAS VEGAS 在 clinicaltrials.gov 上注册(试验标识符 NCT01601223)。