Sandmann Frank G, Davies Nicholas G, Vassall Anna, Edmunds W John, Jit Mark
Centre for Mathematical Modelling of Infectious Diseases, London School of Hygiene & Tropical Medicine, London, UK; Statistics, Modelling and Economics Department, National Infection Service, Public Health England, London, UK.
Centre for Mathematical Modelling of Infectious Diseases, London School of Hygiene & Tropical Medicine, London, UK.
Lancet Infect Dis. 2021 Jul;21(7):962-974. doi: 10.1016/S1473-3099(21)00079-7. Epub 2021 Mar 18.
In response to the COVID-19 pandemic, the UK first adopted physical distancing measures in March, 2020. Vaccines against SARS-CoV-2 became available in December, 2020. We explored the health and economic value of introducing SARS-CoV-2 immunisation alongside physical distancing in the UK to gain insights about possible future scenarios in a post-vaccination era.
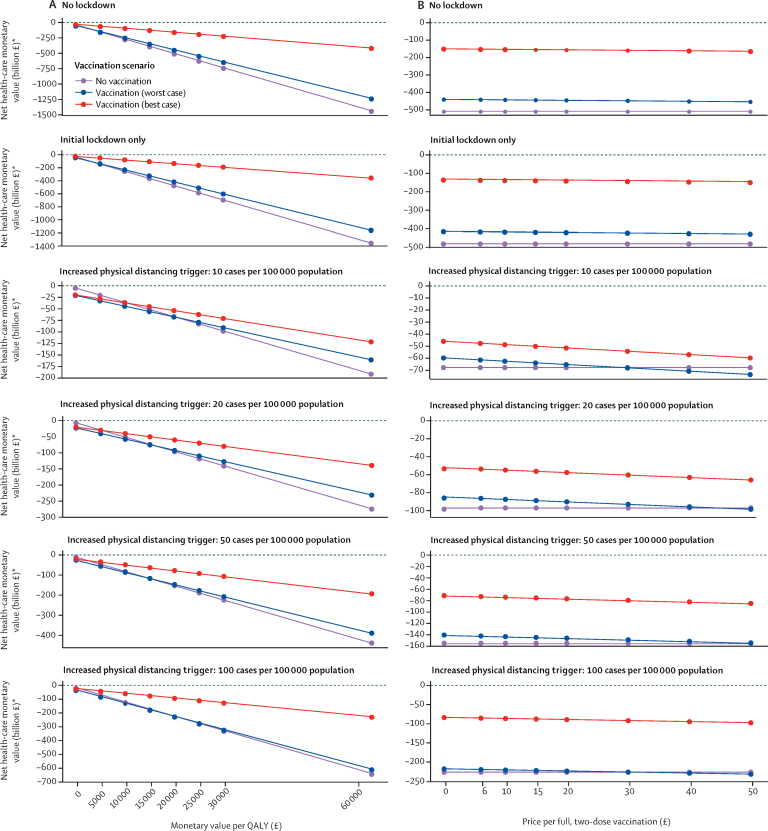
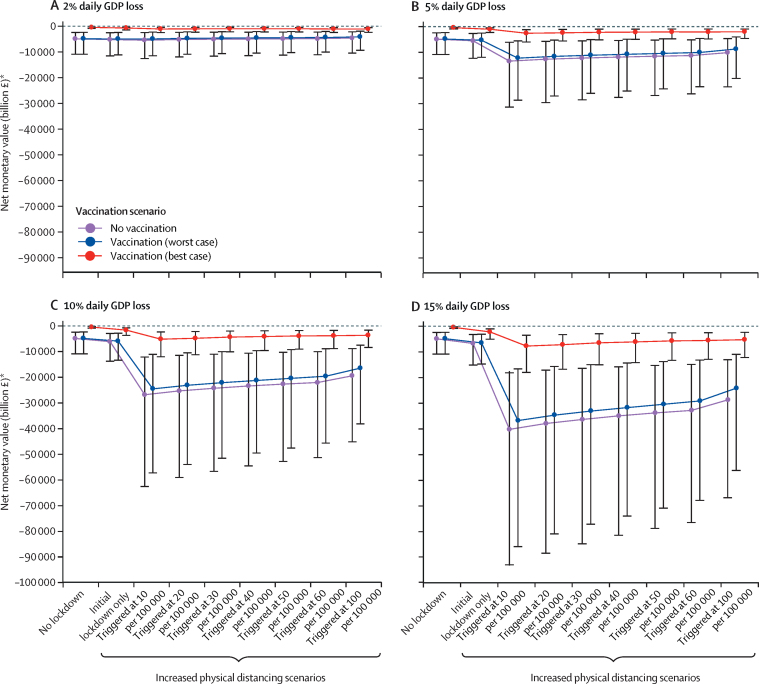
We used an age-structured dynamic transmission and economic model to explore different scenarios of UK mass immunisation programmes over 10 years. We compared vaccinating 75% of individuals aged 15 years or older (and annually revaccinating 50% of individuals aged 15-64 years and 75% of individuals aged 65 years or older) to no vaccination. We assumed either 50% vaccine efficacy against disease and 45-week protection (worst-case scenario) or 95% vaccine efficacy against infection and 3-year protection (best-case scenario). Natural immunity was assumed to wane within 45 weeks. We also explored the additional impact of physical distancing on vaccination by assuming either an initial lockdown followed by voluntary physical distancing, or an initial lockdown followed by increased physical distancing mandated above a certain threshold of incident daily infections. We considered benefits in terms of quality-adjusted life-years (QALYs) and costs, both to the health-care payer and the national economy. We discounted future costs and QALYs at 3·5% annually and assumed a monetary value per QALY of £20 000 and a conservative long-run cost per vaccine dose of £15. We explored and varied these parameters in sensitivity analyses. We expressed the health and economic benefits of each scenario with the net monetary value: QALYs × (monetary value per QALY) - costs.
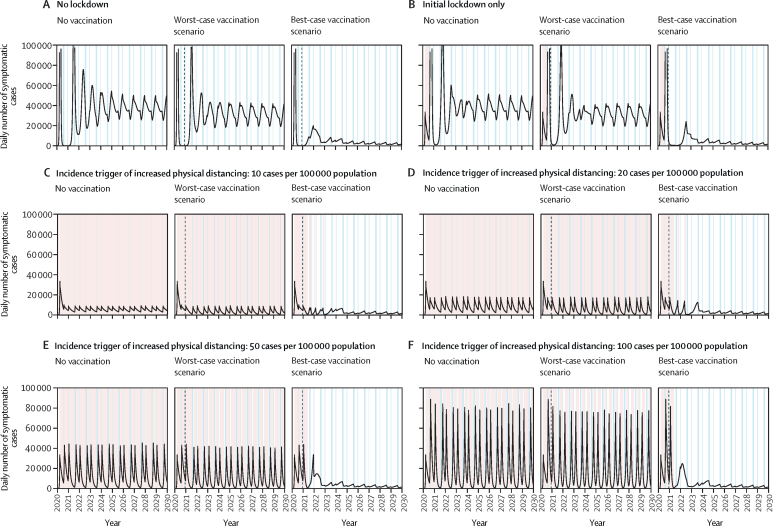
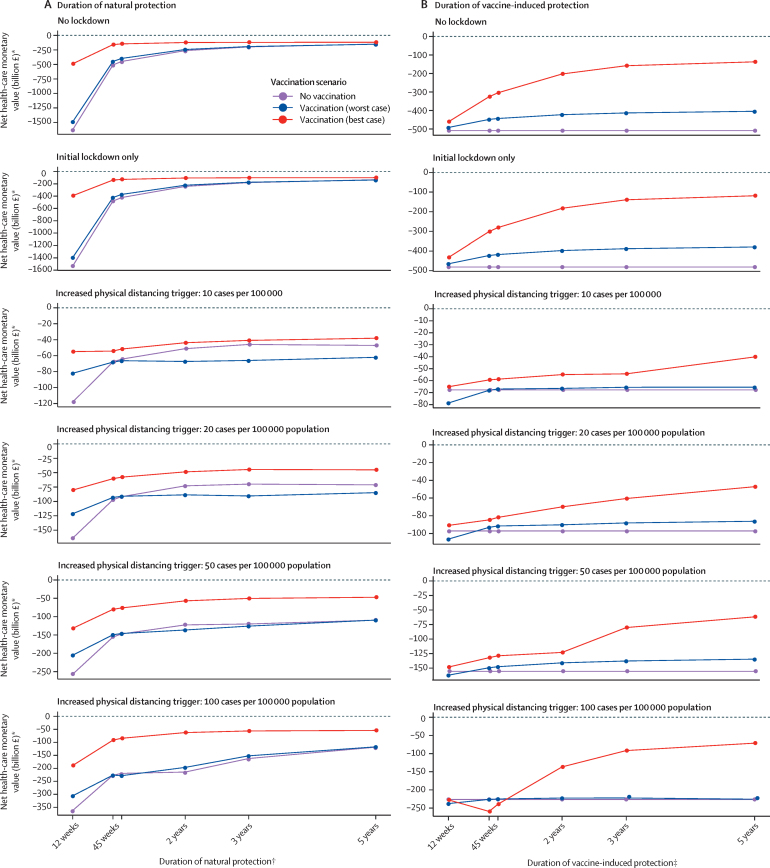
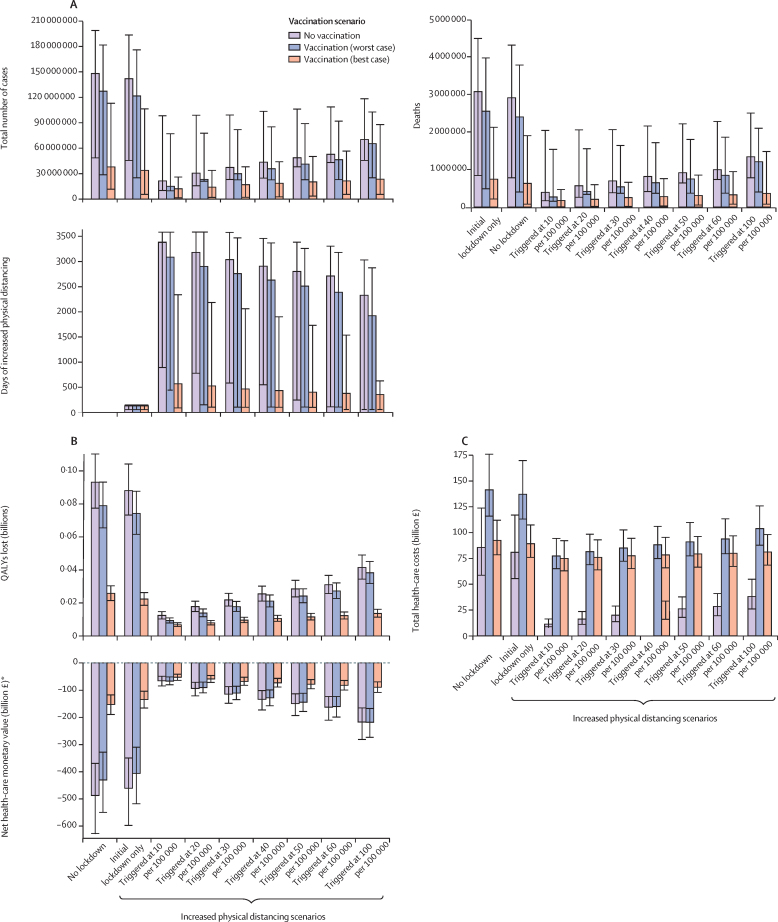
Without the initial lockdown, vaccination, and increased physical distancing, we estimated 148·0 million (95% uncertainty interval 48·5-198·8) COVID-19 cases and 3·1 million (0·84-4·5) deaths would occur in the UK over 10 years. In the best-case scenario, vaccination minimises community transmission without future periods of increased physical distancing, whereas SARS-CoV-2 becomes endemic with biannual epidemics in the worst-case scenario. Ongoing transmission is also expected in intermediate scenarios with vaccine efficacy similar to published clinical trial data. From a health-care perspective, introducing vaccination leads to incremental net monetary values ranging from £12·0 billion to £334·7 billion in the best-case scenario and from -£1·1 billion to £56·9 billion in the worst-case scenario. Incremental net monetary values of increased physical distancing might be negative from a societal perspective if national economy losses are persistent and large.
Our model findings highlight the substantial health and economic value of introducing SARS-CoV-2 vaccination. Smaller outbreaks could continue even with vaccines, but population-wide implementation of increased physical distancing might no longer be justifiable. Our study provides early insights about possible future post-vaccination scenarios from an economic and epidemiological perspective.
National Institute for Health Research, European Commission, Bill & Melinda Gates Foundation.
为应对新冠疫情,英国于2020年3月首次采取了物理距离措施。2020年12月,抗严重急性呼吸综合征冠状病毒2(SARS-CoV-2)疫苗开始可用。我们探讨了在英国将SARS-CoV-2免疫接种与物理距离措施相结合的健康和经济价值,以深入了解疫苗接种后时代可能出现的未来情况。
我们使用了一个按年龄分层的动态传播和经济模型,来探索英国在10年内大规模免疫计划的不同情景。我们将为15岁及以上人群中的75%接种疫苗(并每年为15 - 64岁人群中的50%和65岁及以上人群中的75%再次接种疫苗)与不接种疫苗的情况进行了比较。我们假设疫苗对疾病的效力为50%且提供45周的保护(最坏情况),或对感染的效力为95%且提供3年的保护(最佳情况)。假定自然免疫力在45周内减弱。我们还通过假设两种情况来探讨物理距离措施对疫苗接种的额外影响,一种是最初实施封锁,随后是自愿保持物理距离,另一种是最初实施封锁,随后在每日新增感染病例达到一定阈值后强制实施更严格的物理距离措施。我们考虑了对医疗保健支付方和国民经济在质量调整生命年(QALYs)和成本方面的益处。我们按每年3.5%对未来成本和QALYs进行贴现,并假设每个QALY的货币价值为20000英镑,每剂疫苗的保守长期成本为15英镑。我们在敏感性分析中对这些参数进行了探索和变动。我们用净货币价值来表示每种情景的健康和经济效益:QALYs×(每个QALY的货币价值) - 成本。
如果不采取最初的封锁、疫苗接种以及加强物理距离措施,我们估计在10年内英国将有1.480亿例(95%不确定区间为4850万 - 1.988亿例)新冠病例和310万例(84万 - 450万例)死亡。在最佳情况下,疫苗接种可将社区传播降至最低,且无需在未来进一步加强物理距离措施;而在最坏情况下,SARS-CoV-2将成为地方病,每半年出现一次疫情。在疫苗效力与已发表临床试验数据相似的中间情况下,预计仍会有持续传播。从医疗保健角度来看,在最佳情况下,引入疫苗接种带来的增量净货币价值在120亿英镑至3347亿英镑之间,在最坏情况下则在 - 11亿英镑至569亿英镑之间。如果国民经济损失持续且巨大,从社会角度来看,加强物理距离措施的增量净货币价值可能为负。
我们的模型研究结果凸显了引入SARS-CoV-2疫苗接种的巨大健康和经济价值。即使有疫苗,小规模疫情仍可能继续,但在全国范围内实施更严格的物理距离措施可能不再合理。我们的研究从经济和流行病学角度对疫苗接种后可能出现的未来情况提供了早期见解。
英国国家卫生研究院、欧盟委员会、比尔及梅琳达·盖茨基金会。