Jende Johann M E, Kender Zoltan, Mooshage Christoph, Groener Jan B, Alvarez-Ramos Lucia, Kollmer Jennifer, Juerchott Alexander, Hahn Artur, Heiland Sabine, Nawroth Peter, Bendszus Martin, Kopf Stefan, Kurz Felix T
Department of Neuroradiology, Heidelberg University Hospital, Heidelberg, Germany.
Department of Endocrinology, Diabetology and Clinical Chemistry, Heidelberg University Hospital, Heidelberg, Germany.
Front Neurosci. 2021 Mar 3;15:642589. doi: 10.3389/fnins.2021.642589. eCollection 2021.
Nerve damage in diabetic neuropathy (DN) is assumed to begin in the distal legs with a subsequent progression to hands and arms at later stages. In contrast, recent studies have found that lower limb nerve lesions in DN predominate at the proximal sciatic nerve and that, in the upper limb, nerve functions can be impaired at early stages of DN.
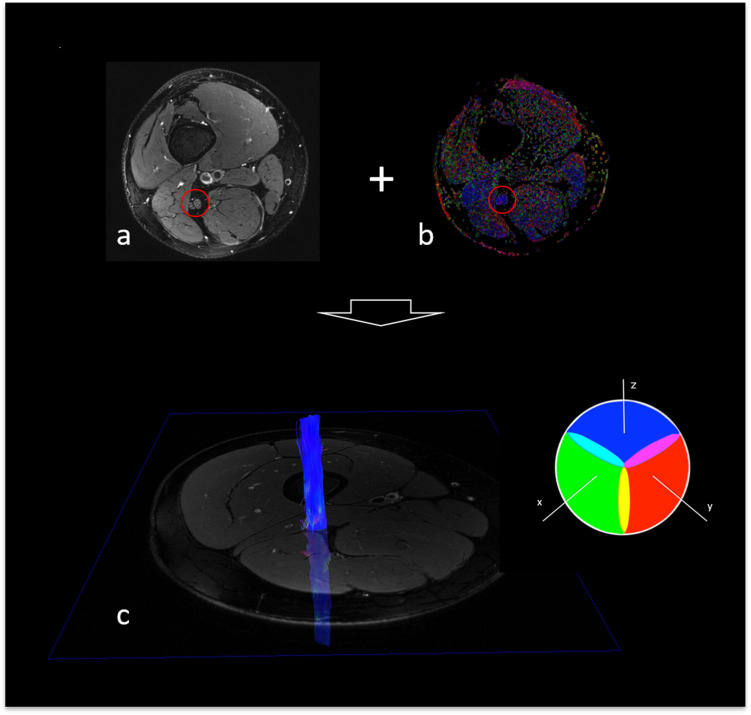
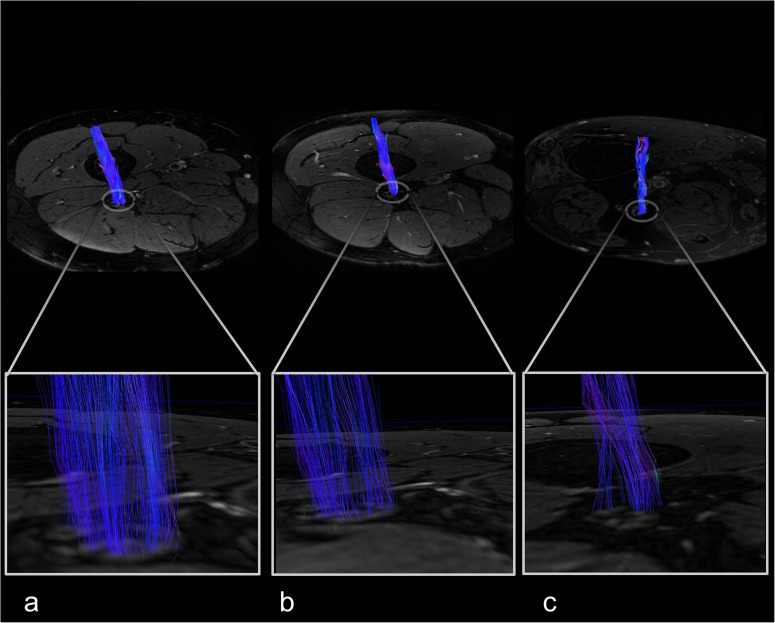
In this prospective, single-center cross-sectional study, participants underwent diffusion-weighted 3 Tesla magnetic resonance neurography in order to calculate the sciatic nerve's fractional anisotropy (FA), a surrogate parameter for structural nerve integrity. Results were correlated with clinical and electrophysiological assessments of the lower limb and an examination of hand function derived from the Purdue Pegboard Test.
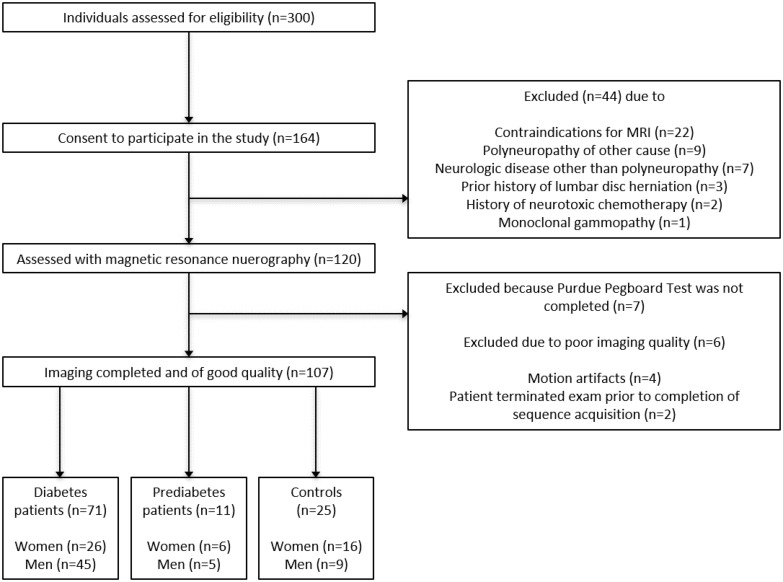
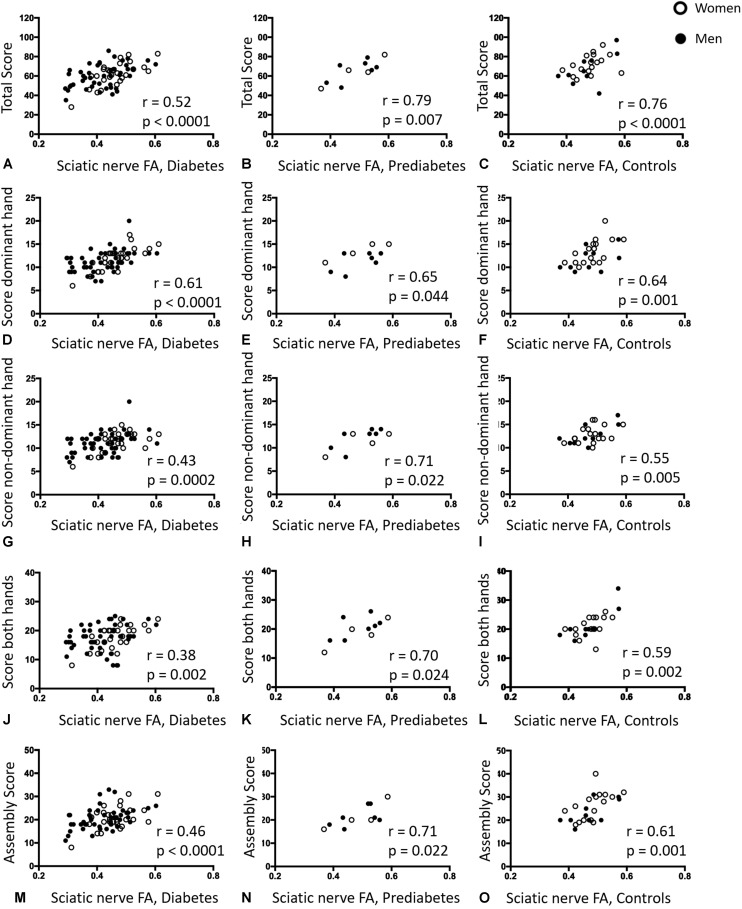
Overall, 71 patients with diabetes, 11 patients with prediabetes and 25 age-matched control subjects took part in this study. In patients with diabetes, the sciatic nerve's FA showed positive correlations with tibial and peroneal nerve conduction velocities ( = 0.62; < 0.001 and = 0.56; < 0.001, respectively), and tibial and peroneal nerve compound motor action potentials ( = 0.62; < 0.001 and = 0.63; < 0.001, respectively). Moreover, the sciatic nerve's FA was correlated with the Pegboard Test results in patients with diabetes ( = 0.52; < 0.001), prediabetes ( = 0.76; < 0.001) and in controls ( = 0.79; = 0.007).
This study is the first to show that the sciatic nerve's FA is a surrogate marker for functional and electrophysiological parameters of both upper and lower limbs in patients with diabetes and prediabetes, suggesting that nerve damage in these patients is not restricted to the level of the symptomatic limbs but rather affects the entire peripheral nervous system.
糖尿病性神经病变(DN)中的神经损伤被认为始于远端腿部,随后在后期发展至手部和手臂。相比之下,最近的研究发现,DN中的下肢神经病变主要发生在近端坐骨神经,并且在上肢,DN早期神经功能就可能受损。
在这项前瞻性、单中心横断面研究中,参与者接受了3特斯拉扩散加权磁共振神经成像,以计算坐骨神经的分数各向异性(FA),这是神经结构完整性的替代参数。结果与下肢的临床和电生理评估以及来自普渡钉板测试的手部功能检查相关。
总体而言,71例糖尿病患者、11例糖尿病前期患者和25例年龄匹配的对照受试者参与了本研究。在糖尿病患者中,坐骨神经的FA与胫神经和腓总神经传导速度呈正相关(分别为r = 0.62;P < 0.001和r = 0.56;P < 0.001),以及与胫神经和腓总神经复合运动动作电位呈正相关(分别为r = 0.62;P < 0.001和r = 0.63;P < 0.001)。此外,坐骨神经的FA与糖尿病患者(r = 0.52;P < 0.001)、糖尿病前期患者(r = 0.76;P < 0.001)和对照组(r = 0.79;P = 0.007)的钉板测试结果相关。
本研究首次表明,坐骨神经的FA是糖尿病和糖尿病前期患者上下肢功能和电生理参数的替代标志物,表明这些患者的神经损伤不仅限于有症状肢体的水平,而是影响整个周围神经系统。