Yan Yuling, Liu Bin, Du Jun, Wang Jing, Jing Xiaodong, Liu Yajie, Deng Songbai, Du Jianlin, She Qiang
Department of Cardiology, The Second Affiliated Hospital of Chongqing Medical University, No. 74, Linjiang Road, Yuzhong District, Chongqing, 400010, China.
ESC Heart Fail. 2021 Jun;8(3):2210-2219. doi: 10.1002/ehf2.13313. Epub 2021 Mar 21.
This study aimed to determine the effects of sodium-glucose cotransporter-2 inhibitor (SGLT2i) in heart failure with reduced ejection fraction (HFrEF), compare the effect of SGLT2i with angiotensin receptor neprilysin inhibitor (ARNI), and find whether combination of SGLT2i and ARNI is better than monotherapy.
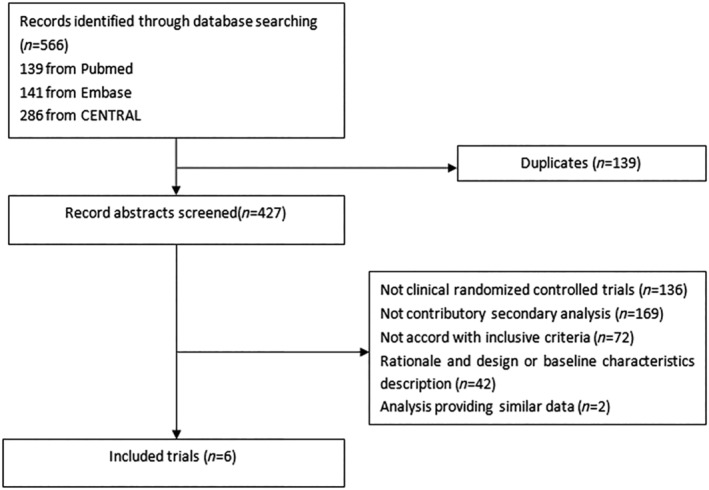
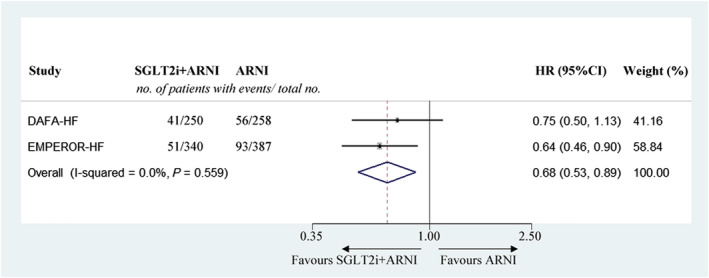
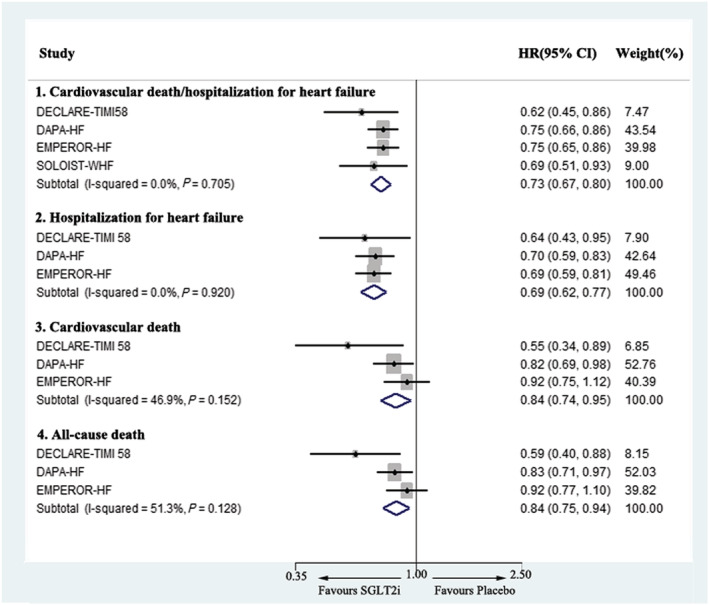
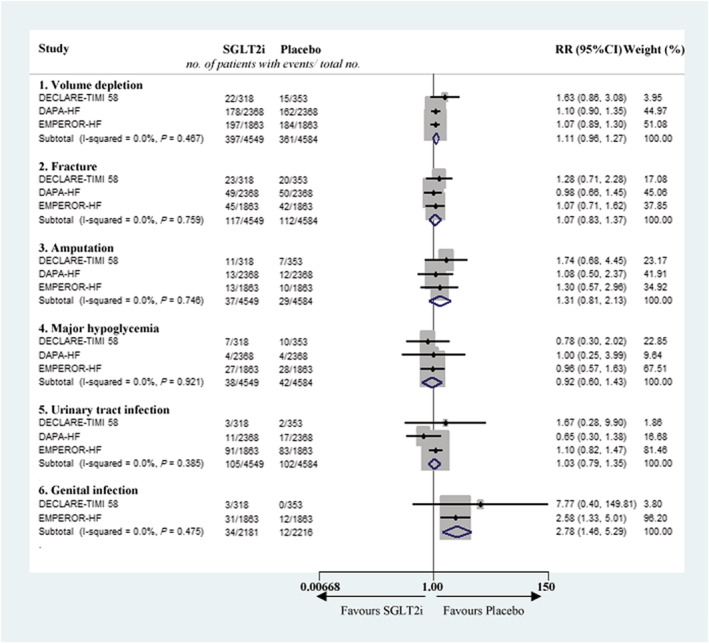
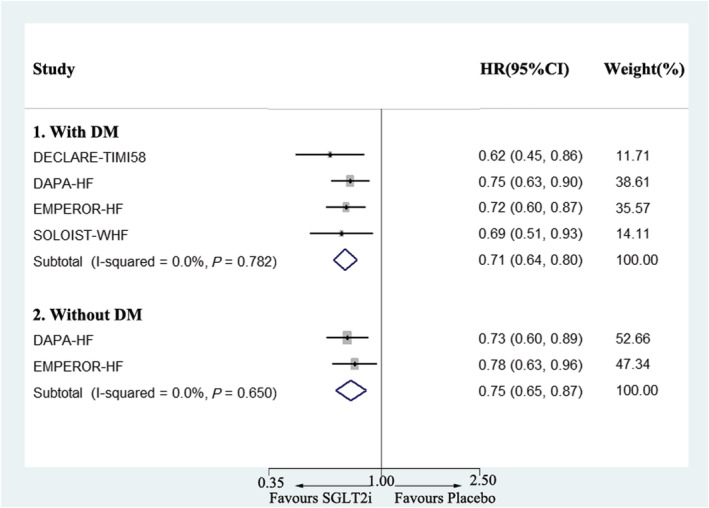
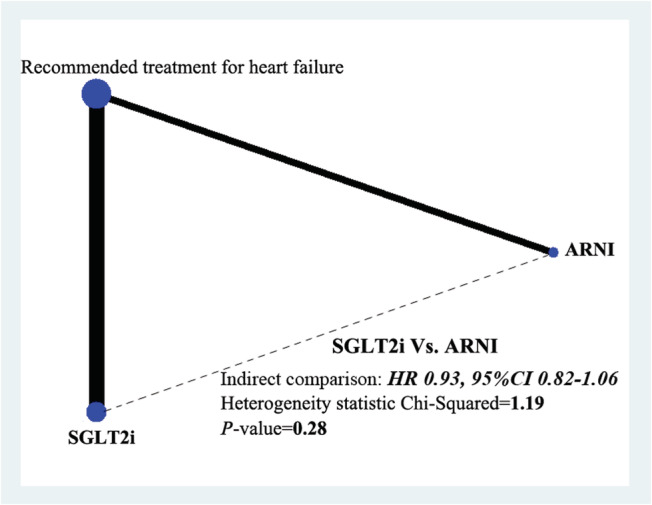
Embase, Medline, and Cochrane Central Registry of Controlled Trials were searched for randomized controlled trials evaluating SGLT2i or ARNI in HFrEF. And a total of six trials were included. SGLT2i was found to significantly reduce the risk of cardiovascular death or hospitalization for heart failure by 27% [hazard ratio (HR) 0.73, 95% confidence interval (CI) 0.67-0.80], hospitalization for heart failure by 31% (HR 0.69, 95% CI 0.62-0.77), cardiovascular death by 16% (HR 0.84, 95% CI 0.74-0.95), and all-cause death by 16% (HR 0.84, 95% CI 0.75-0.94) in HFrEF only with a statistically higher risk of genital infection (risk ratio (RR) 2.78, 95% CI 1.46-5.29). The reduction in cardiovascular death or hospitalization for heart failure was of similar magnitude in patients with or without diabetes mellitus (HR 0.71, 95% CI 0.64-0.80 vs. HR 0.75, 95% CI 0.65-0.87) using SGLT2i. Indirect treatment comparison showed that SGLT2i and ARNI had similar effects on primary outcome (HR 0.93, 95% CI 0.82-1.06). And combination of SGLT2i and ARNI achieved a better prognosis performance (HR 0.68, 95% CI 0.53-0.89) compared with ARNI monotherapy.
SGLT2i could safely reduce cardiovascular death or hospitalization for heart failure in HFrEF regardless of diabetes mellitus status. SGLT2i and ARNI demonstrate similar effects, while combination of SGLT2i and ARNI results in a better cardiovascular protective effect.
本研究旨在确定钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)对射血分数降低的心力衰竭(HFrEF)的影响,比较SGLT2i与血管紧张素受体脑啡肽酶抑制剂(ARNI)的效果,并探究SGLT2i与ARNI联合使用是否优于单一疗法。
检索Embase、Medline和Cochrane对照试验中央注册库,以查找评估SGLT2i或ARNI用于HFrEF的随机对照试验。共纳入六项试验。结果发现,SGLT2i可使HFrEF患者心血管死亡或因心力衰竭住院的风险显著降低27%[风险比(HR)0.73,95%置信区间(CI)0.67 - 0.80],因心力衰竭住院的风险降低31%(HR 0.69,95%CI 0.62 - 0.77),心血管死亡风险降低16%(HR 0.84,95%CI 0.74 - 0.95),全因死亡风险降低16%(HR 0.84,95%CI 0.75 - 0.94),但生殖器感染风险在统计学上显著更高(风险比(RR)2.78,95%CI 1.46 - 5.29)。使用SGLT2i的糖尿病患者和非糖尿病患者在心血管死亡或因心力衰竭住院方面的降低幅度相似(HR 0.71,95%CI 0.64 - 0.80对比HR 0.75,95%CI 0.65 - 0.87)。间接治疗比较显示,SGLT2i和ARNI对主要结局的影响相似(HR 0.93,95%CI 0.82 - 1.06)。与ARNI单一疗法相比,SGLT2i与ARNI联合使用的预后表现更佳(HR 0.68,95%CI 0.53 - 0.89)。
无论糖尿病状态如何,SGLT2i均可安全降低HFrEF患者心血管死亡或因心力衰竭住院的风险。SGLT2i和ARNI效果相似,而SGLT2i与ARNI联合使用具有更好的心血管保护作用。