Pacific Northwest Evidence-Based Practice Center, Medical Informatics and Clinical Epidemiology, the Department of Nurse-Midwifery, School of Nursing, the School of Public Health, Portland State University, and Obstetrics and Gynecology, Oregon Health & Science University, Portland, Oregon; and Aggregate Analytics, Fircrest, Washington.
Obstet Gynecol. 2021 Jun 1;137(6):1091-1101. doi: 10.1097/AOG.0000000000004382.
To assess the comparative effectiveness and potential harms of cervical ripening in the outpatient compared with the inpatient setting, or different methods of ripening in the outpatient setting alone.
Searches for articles in English included MEDLINE, EMBASE, CINAHL, Cochrane Library, ClinicalTrials.gov, and reference lists (up to August 2020).
Using predefined criteria and DistillerSR software, 10,853 citations were dual-reviewed for randomized controlled trials (RCTs) and cohort studies of outpatient cervical ripening using prostaglandins and mechanical methods in pregnant women at or beyond 37 weeks of gestation.
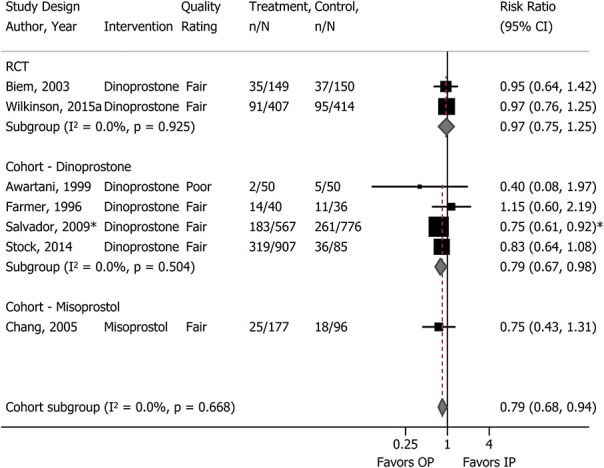
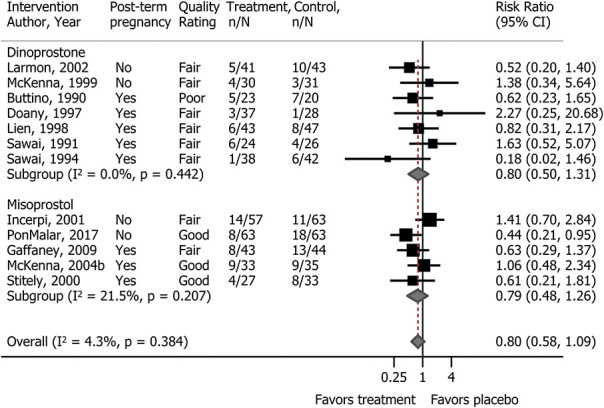
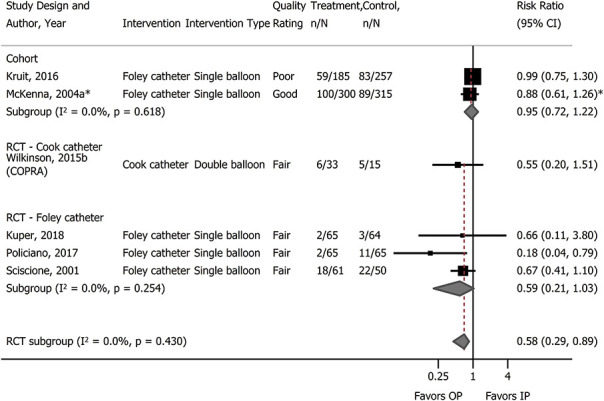
TABULATION, INTEGRATION, AND RESULTS: Using prespecified criteria, study data abstraction and risk of bias assessment were conducted by two reviewers, random-effects meta-analyses were conducted and strength of evidence was assessed. We included 30 RCTs and 10 cohort studies (N=9,618) most generalizable to women aged 25-30 years with low-risk pregnancies. All findings were low or insufficient strength of evidence and not statistically significant. Incidence of cesarean delivery was not different for any comparison of inpatient and outpatient settings, or comparisons of different methods in the outpatient setting (most evidence available for single-balloon catheters and dinoprostone). Harms were inconsistently reported or inadequately defined. Differences were not found for neonatal infection (eg, sepsis) with outpatient compared with inpatient dinoprostone, birth trauma (eg, cephalohematoma) with outpatient compared with inpatient single-balloon catheter, shoulder dystocia with outpatient dinoprostone compared with placebo, maternal infection (eg, chorioamnionitis) with outpatient compared with inpatient single-balloon catheters or outpatient prostaglandins compared with placebo, and postpartum hemorrhage with outpatient catheter compared with inpatient dinoprostone. Evidence on misoprostol, hygroscopic dilators, and other outcomes (eg, perinatal mortality and time to vaginal birth) was insufficient.
In women with low-risk pregnancies, outpatient cervical ripening with dinoprostone or single-balloon catheters did not increase cesarean deliveries. Although there were no clear differences in harms when comparing outpatient with inpatient cervical ripening, the certainty of evidence is low or insufficient to draw definitive conclusions.
PROSPERO, CRD42020167406.
评估门诊与住院环境下,或门诊环境下单独使用不同软化宫颈方法进行宫颈成熟时的比较效果和潜在危害。
英文检索包括 MEDLINE、EMBASE、CINAHL、 Cochrane 图书馆、ClinicalTrials.gov 和参考文献(截至 2020 年 8 月)。
使用预设标准和 DistillerSR 软件,对在妊娠 37 周或以上的低危孕妇中使用前列腺素和机械方法进行门诊宫颈成熟的随机对照试验(RCT)和队列研究的 10853 篇引文进行双重审查。
表格、综合和结果:使用预设标准,由两名审查员进行研究数据提取和偏倚风险评估,进行随机效应荟萃分析并评估证据强度。我们纳入了 30 项 RCT 和 10 项队列研究(N=9618),这些研究最适用于年龄在 25-30 岁、低危妊娠的女性。所有研究结果的证据强度均较低或不足,且无统计学意义。与门诊相比,住院和门诊环境之间的剖宫产发生率没有差异,门诊环境下不同方法之间的比较也没有差异(单球囊导管和地诺前列酮的证据最多)。危害的报告不一致或定义不充分。与门诊相比,门诊地诺前列酮组新生儿感染(如败血症)和门诊单球囊导管组分娩创伤(如头颅血肿)的差异无统计学意义,门诊地诺前列酮组肩难产与安慰剂相比,门诊组与安慰剂相比,产妇感染(如绒毛膜羊膜炎)与门诊单球囊导管或门诊前列腺素与安慰剂相比,门诊导管与住院地诺前列酮相比,产后出血。关于米索前列醇、吸湿扩张器和其他结局(如围产儿死亡率和阴道分娩时间)的证据不足。
在低危妊娠的女性中,门诊使用地诺前列酮或单球囊导管进行宫颈成熟不会增加剖宫产率。尽管比较门诊与住院宫颈成熟时,危害无明显差异,但证据的确定性较低或不足,无法得出明确结论。
PROSPERO,CRD42020167406。