Department of Trauma Surgery, University Medical Center Regensburg, Franz-Josef-Strauss-Allee 11, 93053, Regensburg, Germany.
Sporthopaedicum, Regensburg, Straubing, Germany.
Knee Surg Sports Traumatol Arthrosc. 2021 Oct;29(10):3149-3158. doi: 10.1007/s00167-021-06525-8. Epub 2021 Mar 23.
Septic arthritis is a significant complication following arthroscopic surgery, with an estimated overall incidence of less than 1%. Despite the low incidence, an appropriate diagnostic and therapeutic pathway is required to avoid serious long-term consequences, eradicate the infection, and ensure good treatment outcomes. The aim of this current review article is to summarize evidence-based literature regarding diagnostic and therapeutic options of post-operative septic arthritis after arthroscopy.
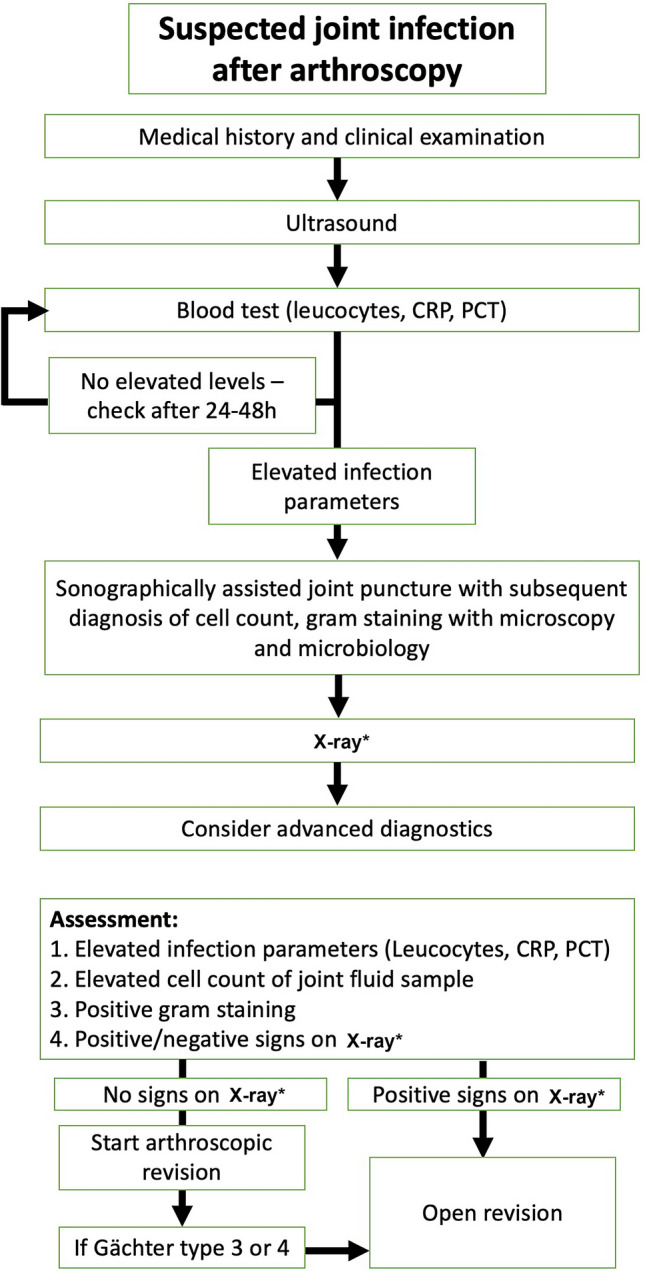
Through a literature review, up-to-date treatment algorithms and therapies have been identified. Additionally, a supportive new algorithm is proposed for diagnosis and treatment of suspected septic arthritis following arthroscopic intervention.
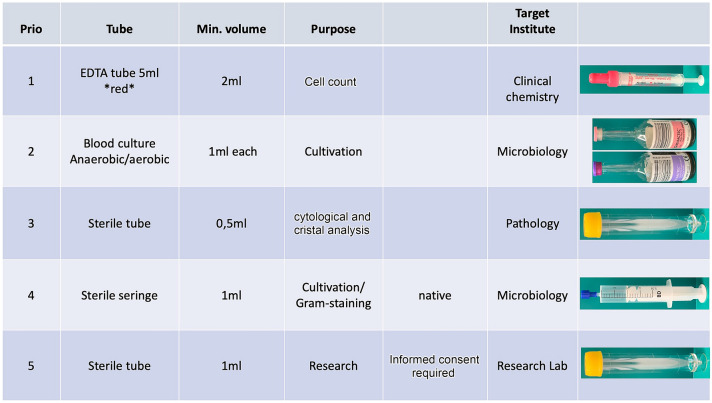
A major challenge in diagnostics is the differentiation of the post-operative status between a non-infected hyperinflammatory joint versus septic arthritis, due to clinical symptoms, (e.g., rubor, calor, or tumor) can appear identical. Therefore, joint puncture for microbiological evaluation, especially for fast leukocyte cell-count diagnostics, is advocated. A cell count of more than 20.000 leukocyte/µl with more than 70% of polymorphonuclear cells is the generally accepted threshold for septic arthritis.
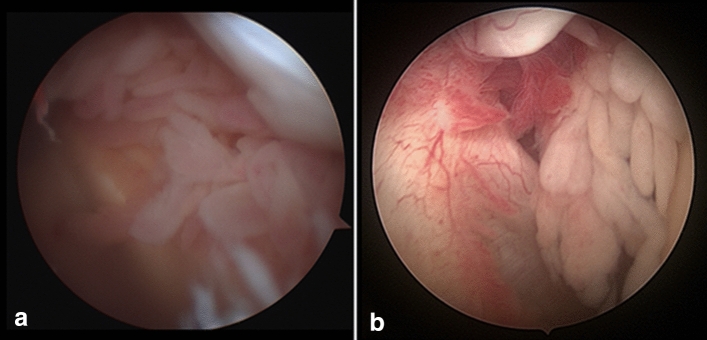
The therapy is based on arthroscopic or open surgical debridement for synovectomy and irrigation of the joint, in combination with an adequate antibiotic therapy for 6-12 weeks. Removal of indwelling hardware, such as interference screws for ACL repair or anchors for rotator cuff repair, is recommended in chronic cases.
IV.
关节镜手术后发生的化脓性关节炎是一种严重的并发症,其总体发病率估计不到 1%。尽管发病率较低,但仍需要采取适当的诊断和治疗途径,以避免严重的长期后果,消除感染,并确保良好的治疗效果。本文旨在总结有关关节镜术后化脓性关节炎的诊断和治疗选择的循证文献。
通过文献回顾,确定了最新的治疗方案和治疗方法。此外,还提出了一种支持性的新算法,用于诊断和治疗关节镜介入后疑似化脓性关节炎。
诊断的一个主要挑战是区分术后非感染性炎症关节与化脓性关节炎之间的状态,因为临床症状(如红肿、发热或肿胀)可能相同。因此,提倡进行关节穿刺以进行微生物评估,特别是快速白细胞细胞计数诊断。白细胞计数超过 20,000/μl,其中多形核细胞超过 70%是化脓性关节炎的公认阈值。
治疗方法基于关节镜或开放性滑膜切除术和关节冲洗,结合 6-12 周的适当抗生素治疗。在慢性病例中,建议取出留置的硬件,如 ACL 修复的干扰螺钉或肩袖修复的锚钉。
IV。