Department of Neurosurgery, Faculty of Medicine, Heinrich-Heine-University, Düsseldorf, Germany.
Department of Neurosurgery, Helsinki University Hospital, University of Helsinki, Helsinki, Finland.
Front Immunol. 2021 Mar 8;12:630381. doi: 10.3389/fimmu.2021.630381. eCollection 2021.
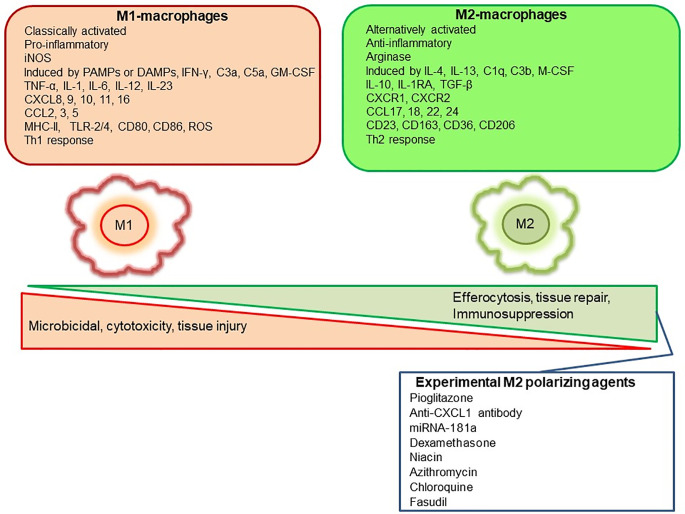
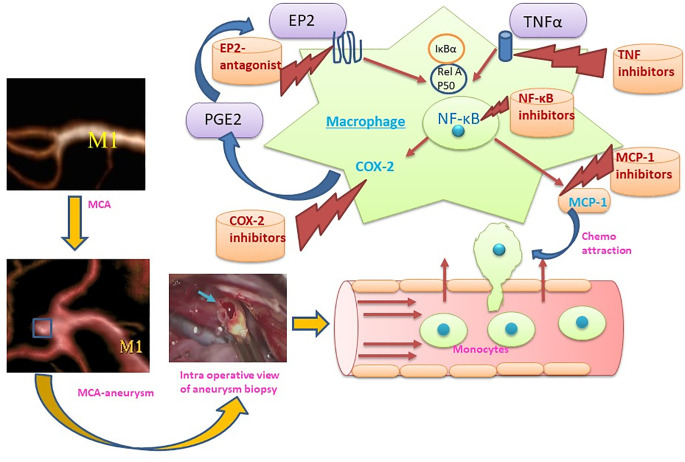
Aneurysmal subarachnoid hemorrhage (aSAH) is a highly fatal and morbid type of hemorrhagic strokes. Intracranial aneurysms (ICAs) rupture cause subarachnoid hemorrhage. ICAs formation, growth and rupture involves cellular and molecular inflammation. Macrophages orchestrate inflammation in the wall of ICAs. Macrophages generally polarize either into classical inflammatory (M1) or alternatively-activated anti-inflammatory (M2)-phenotype. Macrophage infiltration and polarization toward M1-phenotype increases the risk of aneurysm rupture. Strategies that deplete, inhibit infiltration, ameliorate macrophage inflammation or polarize to M2-type protect against ICAs rupture. However, clinical translational data is still lacking. This review summarizes the contribution of macrophage led inflammation in the aneurysm wall and discuss pharmacological strategies to modulate the macrophageal response during ICAs formation and rupture.
颅内动脉瘤破裂导致蛛网膜下腔出血。细胞和分子炎症参与颅内动脉瘤的形成、生长和破裂。巨噬细胞在颅内动脉瘤壁炎症中起协调作用。巨噬细胞通常极化为经典炎症(M1)或替代激活的抗炎(M2)表型。巨噬细胞浸润和向 M1 表型极化增加了动脉瘤破裂的风险。消耗、抑制浸润、改善巨噬细胞炎症或向 M2 型极化的策略可预防颅内动脉瘤破裂。然而,临床转化数据仍然缺乏。本文综述了巨噬细胞引发的炎症在动脉瘤壁中的作用,并讨论了在颅内动脉瘤形成和破裂过程中调节巨噬细胞反应的药理学策略。