Chan Vinson Wai-Shun, Wong Chris Ho Ming, Yuan Yuhong, Teoh Jeremy Yuen-Chun
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds, UK.
Department of Surgery, Prince of Wales Hospital, Hong Kong, China.
Arab J Urol. 2020 Jul 27;19(1):37-45. doi: 10.1080/2090598X.2020.1791563.
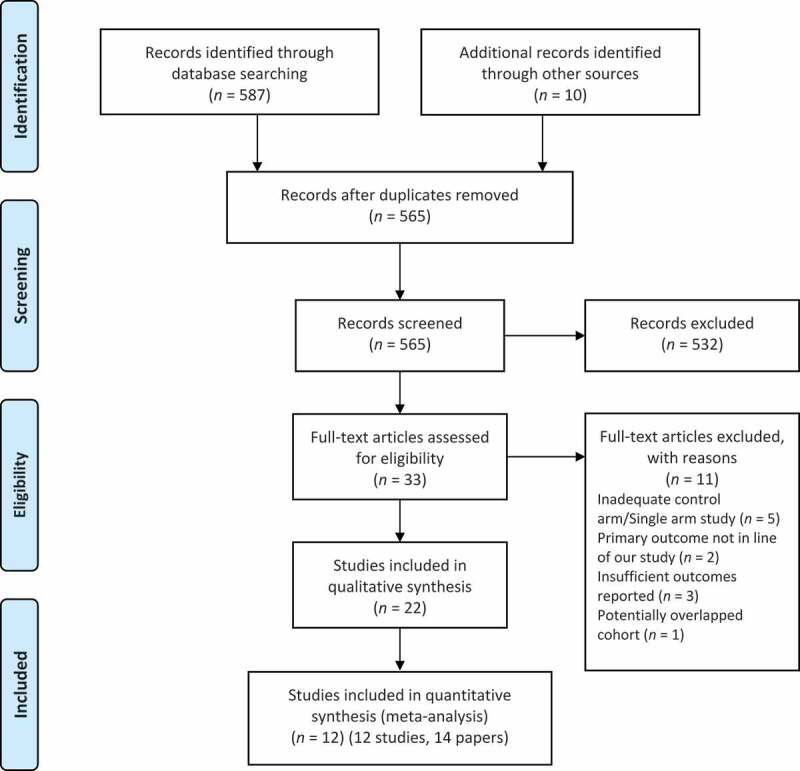
To perform a systematic review, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement, investigating the role of lymph node dissection (LND) during nephroureterectomy (NU) for upper tract urothelial carcinoma (UTUC); focussing on survival and complication outcomes.
A comprehensive systematic search was completed using a combination of Medical Subject Headings terms and keywords related to UTUC and LND on multiple databases. Meta-analyses were performed when outcomes were reported under the same definition in two or more studies. Where meta-analysis was not possible, outcomes were reviewed in a narrative manner.
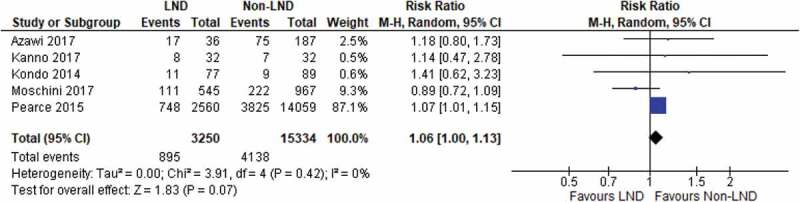
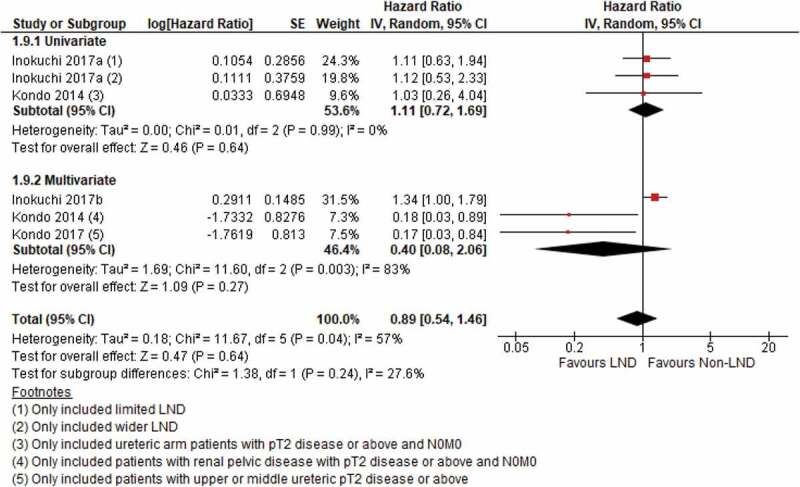
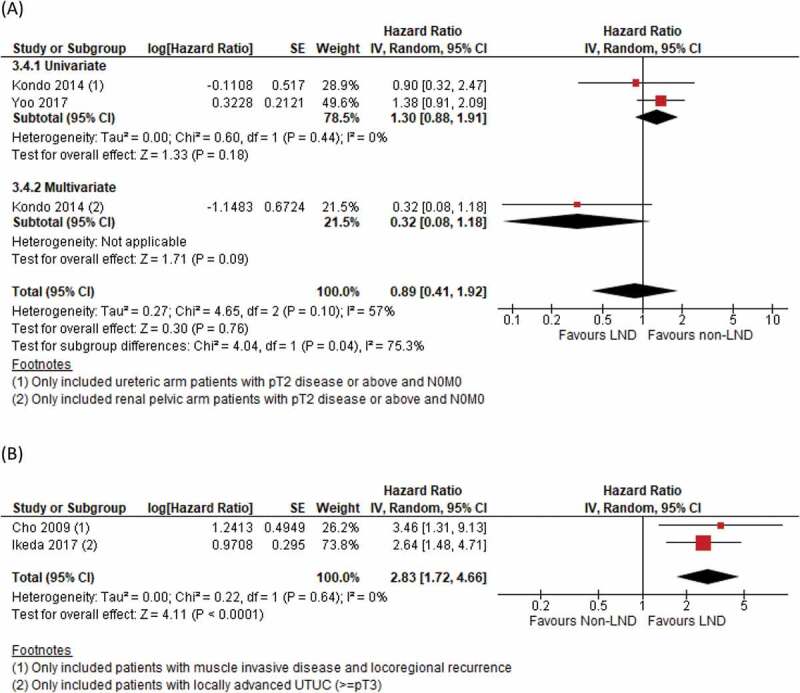
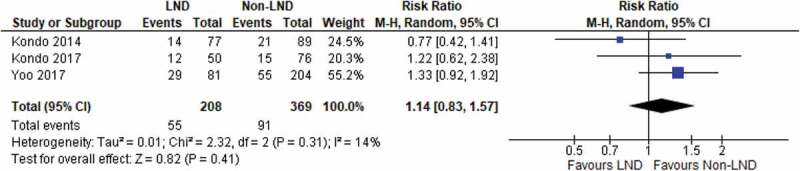
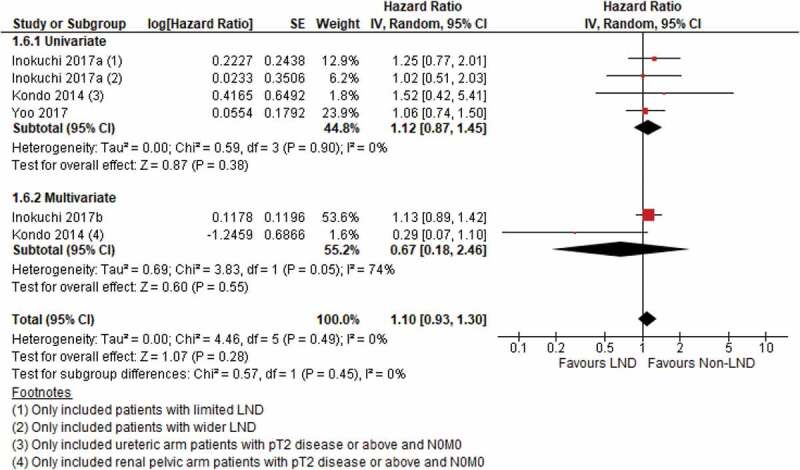
A total of 21 studies were included in the qualitative analysis and 11 cohort studies in the quantitative analysis. Our review did not detect significant improvement in recurrence-free survival (RFS) (hazard ratio [HR] 0.89, 95% confidence interval [CI] 0.41-1.92), cancer-specific survival (CSS) (HR 0.89, 95% CI 0.54-1.46) and overall survival (OS) (HR 1.10, 95% CI 0.93-1.30). However, when focussing on studies only including patients with pT2/pT3 UTUC, not performing LND significantly worsened RFS (HR 2.83, 95% CI 1.72-4.66). Reports of removing more than eight lymph nodes may also provide prognostic benefits in pN0 patients. The performance of LND was not associated with a higher rate of postoperative complications (risk ratio 1.06, 95% CI 1.00-1.13).
Overall, LND did not provide additional benefit in RFS, CSS and OS. However, there was a potential benefit in RFS in patients with muscle-invasive and advanced UTUC. LND was also not associated with increased risks of postoperative complications. CIS: carcinoma ; CSS: cancer-specific survival; HR: hazard ratio; LND: lymph node dissection; NU: nephroureterectomy; OS: overall survival; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RFS: recurrence-free survival; RoB, risk of bias; RR: risk ratio; (UT)UC: (upper tract) urothelial carcinoma.
根据系统评价与Meta分析的首选报告项目(PRISMA)声明进行一项系统评价,探讨淋巴结清扫术(LND)在上尿路尿路上皮癌(UTUC)肾输尿管切除术(NU)中的作用;重点关注生存和并发症结局。
在多个数据库中结合使用与UTUC和LND相关的医学主题词和关键词,完成全面的系统检索。当两项或更多研究在相同定义下报告结局时,进行Meta分析。若无法进行Meta分析,则以叙述方式回顾结局。
定性分析共纳入21项研究,定量分析纳入11项队列研究。我们的评价未发现无复发生存期(RFS)(风险比[HR]0.89,95%置信区间[CI]0.41 - 1.92)、癌症特异性生存期(CSS)(HR 0.89,95%CI 0.54 - 1.46)和总生存期(OS)(HR 1.10,95%CI 0.93 - 1.30)有显著改善。然而,仅关注纳入pT2/pT3 UTUC患者的研究时,未进行LND会显著恶化RFS(HR 2.83,95%CI 1.72 - 4.66)。切除超过8个淋巴结的报告对pN0患者也可能具有预后益处。LND的实施与术后并发症发生率较高无关(风险比1.06,95%CI 1.00 - 1.13)。
总体而言,LND在RFS、CSS和OS方面未提供额外益处。然而,对于肌层浸润性和晚期UTUC患者,LND在RFS方面可能有益。LND也与术后并发症风险增加无关。CIS:癌;CSS:癌症特异性生存期;HR:风险比;LND:淋巴结清扫术;NU:肾输尿管切除术;OS:总生存期;PRISMA:系统评价与Meta分析的首选报告项目;RFS:无复发生存期;RoB:偏倚风险;RR:风险比;(UT)UC:(上尿路)尿路上皮癌