Pasqui Edoardo, de Donato Gianmarco, Alba Giuseppe, Brancaccio Brenda, Panzano Claudia, Cappelli Alessandro, Setacci Carlo, Palasciano Giancarlo
Vascular Surgery Unit, Department of Medicine, Surgery, and Neuroscience, University of Siena, Siena, Italy.
Front Surg. 2021 Mar 8;8:646204. doi: 10.3389/fsurg.2021.646204. eCollection 2021.
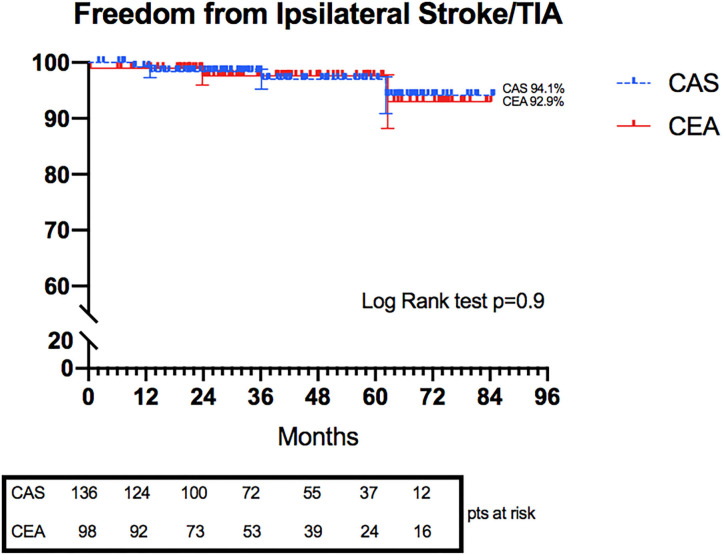
The role of carotid revascularization in women remains intensely debated because of the lower benefit and higher perioperative risks concerning the male counterpart. Carotid artery endarterectomy (CEA) and stenting (CAS) represent the two most valuable stroke prevention techniques due to large vessel disease. This study investigates the early and late outcomes in female sex in a real-world everyday clinical practice. Data were retrospectively analyzed from a single-center database prospectively compiled. A total of 234 procedures, both symptomatic and asymptomatic, were identified (98 CEAs and 136 CASs). Perioperative risks of death, cerebral ischemic events, and local complications were analyzed and compared between the two groups. Long-term outcomes were evaluated in overall survival, freedom from ipsilateral stroke/transient ischemic attack, and freedom from restenosis (>50%) and reintervention. Women who underwent CAS and CEA did not differ in perioperative ischemic cerebral events (2.2 vs. 0%, = 0.26) and death (0.8 vs. 0%, = 1). Other perioperative and 30-day outcomes were similarly distributed within the two groups. Kaplan-Meier curves between CAS and CEA groups highlighted no statistical differences at 6 years in overall survival (77.4 vs. 77.1%, = 0.47) of ipsilateral stroke/transient ischemic attack (94.1 vs. 92.9%, = 0.9). Conversely, significant differences were showed in 6 years freedom from restenosis (93.1 vs. 83.3%, = 0.03) and reinterventions (97.7 vs. 87.8%, = 0.015). Our results revealed that both CEA and CAS have acceptable perioperative risk in women. Long-term outcomes highlighted favorable indications for both procedures, especially for CAS, which seemed to be an excellent alternative to CEA in female patients when performed by well-trained operators.
由于与男性相比获益较低且围手术期风险较高,颈动脉血运重建在女性中的作用仍存在激烈争论。由于大血管疾病,颈动脉内膜切除术(CEA)和支架置入术(CAS)是两种最有价值的预防中风技术。本研究在日常临床实践的真实环境中调查了女性患者的早期和晚期结局。数据来自前瞻性汇编的单中心数据库,进行回顾性分析。共识别出234例手术,包括有症状和无症状的(98例CEA和136例CAS)。分析并比较了两组围手术期的死亡、脑缺血事件和局部并发症风险。评估了总体生存、同侧无中风/短暂性脑缺血发作以及无再狭窄(>50%)和再次干预的长期结局。接受CAS和CEA的女性在围手术期缺血性脑事件(2.2%对0%,P = 0.26)和死亡(0.8%对0%,P = 1)方面无差异。其他围手术期和30天结局在两组中分布相似。CAS组和CEA组之间的Kaplan-Meier曲线显示,6年时总体生存(77.4%对77.1%,P = 0.47)和同侧中风/短暂性脑缺血发作(94.1%对92.9%,P = 0.9)无统计学差异。相反,6年时无再狭窄(93.1%对83.3%,P = 0.03)和再次干预(97.7%对87.8%,P = 0.015)存在显著差异。我们的结果显示,CEA和CAS在女性中的围手术期风险均可接受。长期结局突出了两种手术的良好指征,尤其是CAS,由训练有素的操作者进行时,似乎是女性患者中CEA的极佳替代方案。