Division of Cardiology Department of Medicine Emory Clinical Cardiovascular Research InstituteEmory University School of Medicine Atlanta GA.
Department of Biostatistics and Bioinformatics Rollins School of Public Health Emory University Atlanta GA.
J Am Heart Assoc. 2021 Apr 6;10(7):e020019. doi: 10.1161/JAHA.120.020019. Epub 2021 Mar 25.
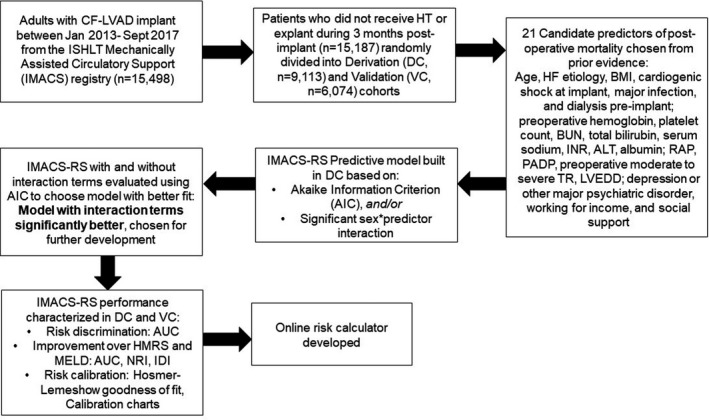
Background Prior studies have shown that women have worse 3-month survival after receiving a left ventricular assist device compared with men. Currently used prognostic scores, including the Heartmate II Risk Score, do not account for the increased residual risk in women. We used the IMACS (International Society for Heart and Lung Transplantation Mechanically Assisted Circulatory Support) registry to create and validate a sex-specific risk score for early mortality in left ventricular assist device recipients. Methods and Results Adult patients with a continuous-flow LVAD from the IMACS registry were randomly divided into a derivation cohort (DC; n=9113; 21% female) and a validation cohort (VC; n=6074; 21% female). The IMACS Risk Score was developed in the DC to predict 3-month mortality, from preoperative candidate predictors selected using the Akaike information criterion, or significant sex × variable interaction. In the DC, age, cardiogenic shock at implantation, body mass index, blood urea nitrogen, bilirubin, hemoglobin, albumin, platelet count, left ventricular end-diastolic diameter, tricuspid regurgitation, dialysis, and major infection before implantation were retained as significant predictors of 3-month mortality. There was significant ischemic heart failure × sex and platelet count × sex interaction. For each quartile increase in IMACS risk score, men (odds ratio [OR], 1.86; 95% CI, 1.74-2.00; <0.0001), and women (OR, 1.93; 95% CI, 1.47-2.59; <0.0001) had higher odds of 3-month mortality. The IMACS risk score represented a significant improvement over Heartmate II Risk Score (IMACS risk score area under the receiver operating characteristic curve: men: DC, 0.71; 95% CI, 0.69-0.73; VC, 0.69; 95% CI, 0.66-0.72; women: DC, 0.73; 95% CI, 0.70-0.77; VC, 0.71 [95% CI, 0.66-0.76; <0.01 for improvement in receiver operating characteristic) and provided excellent risk calibration in both sexes. Removal of sex-specific interaction terms resulted in significant loss of model fit. Conclusions A sex-specific risk score provides excellent risk prediction in LVAD recipients.
先前的研究表明,与男性相比,女性在接受左心室辅助装置治疗后 3 个月的生存率更差。目前使用的预后评分,包括 Heartmate II 风险评分,并没有考虑到女性的剩余风险增加。我们使用国际心肺移植协会(International Society for Heart and Lung Transplantation)机械循环支持(Mechanically Assisted Circulatory Support)登记处的 IMACS 来创建和验证一个用于预测左心室辅助装置接受者早期死亡率的性别特异性风险评分。
来自 IMACS 登记处的成年患者,使用连续流左心室辅助装置,随机分为推导队列(DC;n=9113;21%为女性)和验证队列(VC;n=6074;21%为女性)。使用 DC 中的 IMACS 风险评分来预测 3 个月死亡率,从使用赤池信息量准则(Akaike information criterion)选择的术前候选预测因子中选择,或者显著的性别×变量相互作用。在 DC 中,年龄、植入时心源性休克、体重指数、血尿素氮、胆红素、血红蛋白、白蛋白、血小板计数、左心室舒张末期直径、三尖瓣反流、植入前透析和主要感染保留为 3 个月死亡率的显著预测因子。存在显著的缺血性心力衰竭×性别和血小板计数×性别相互作用。对于 IMACS 风险评分每增加一个四分位,男性(比值比 [OR],1.86;95%置信区间 [CI],1.74-2.00;<0.0001)和女性(OR,1.93;95% CI,1.47-2.59;<0.0001)的 3 个月死亡率更高。IMACS 风险评分与 Heartmate II 风险评分相比有显著改善(IMACS 风险评分的接收者操作特征曲线下面积:男性:DC,0.71;95%CI,0.69-0.73;VC,0.69;95%CI,0.66-0.72;女性:DC,0.73;95%CI,0.70-0.77;VC,0.71[95%CI,0.66-0.76;改善的接收者操作特征的差异<0.01),并为两性提供了极好的风险校准。去除性别特异性相互作用项会导致模型拟合显著丢失。
一个性别特异性风险评分在左心室辅助装置接受者中提供了极好的风险预测。