Nwachuku Enyinna, Duehr James, Pease Matthew W, Lunsford L Dade, Monaco Edward A
Department of Neurosurgery, University of Pittsburgh Medical Center, Pennsylvania, United States.
Department of School of Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania, United States.
Surg Neurol Int. 2021 Mar 8;12:86. doi: 10.25259/SNI_562_2020. eCollection 2021.
Gamma Knife stereotactic radiosurgery (GKRS) facilitates precisely focused radiation to an intracranial target while minimizing substantial off-target radiation in the surrounding normal tissue. Meningiomas attached to or invading the superior sagittal sinus may result in sinus occlusion and are often impossible to completely resect safely. The authors describe successful management of a patient with a meningioma located completely inside the posterior aspect of the superior sagittal sinus.
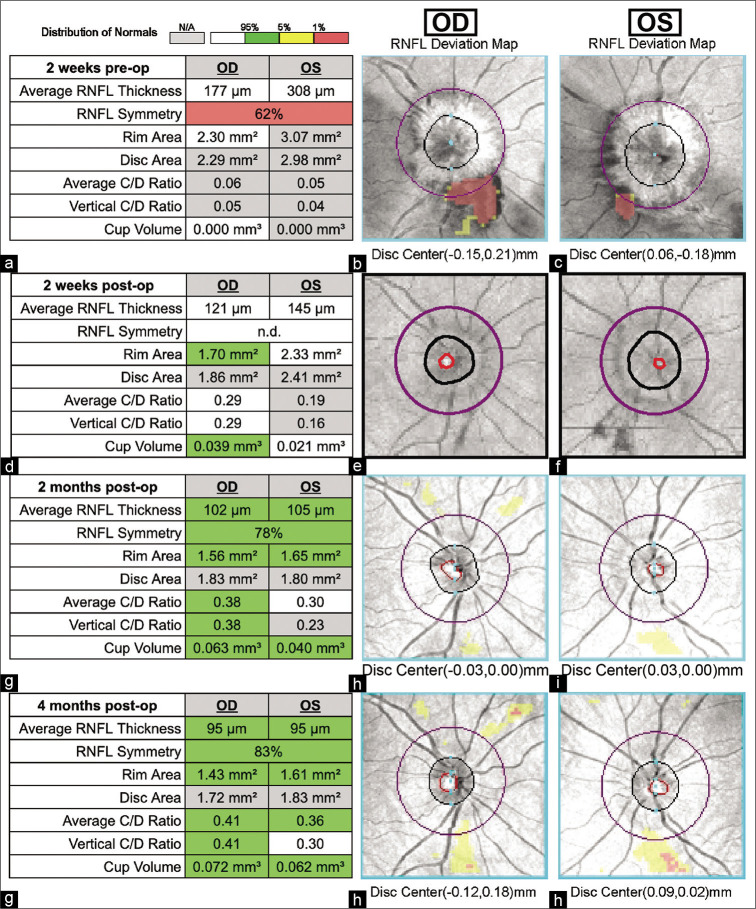
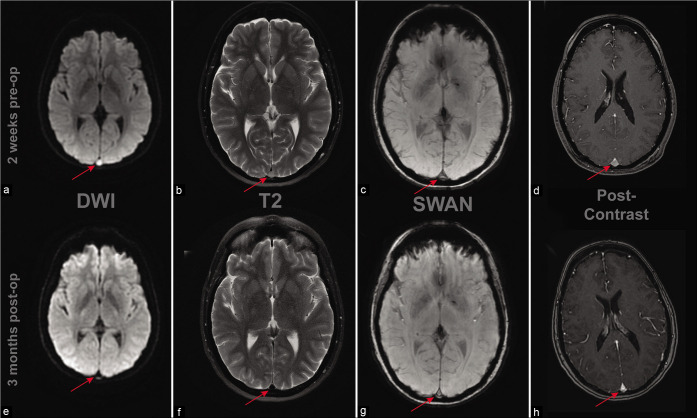
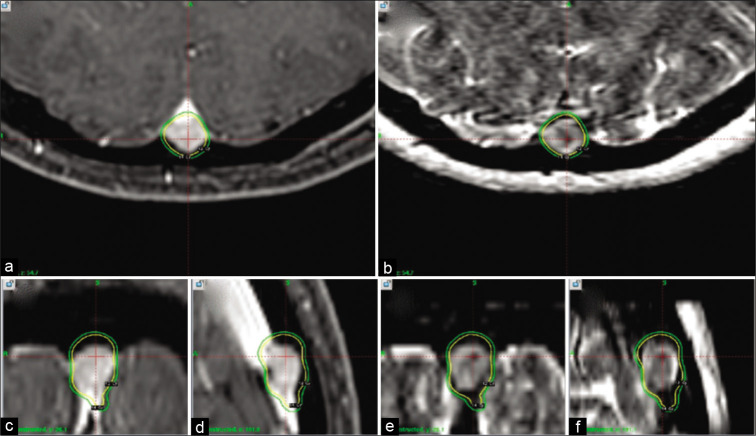
A 46-year-old woman presented to the emergency department with progressive generalized headaches accompanied by worsening vision. The patient underwent a diagnostic brain magnetic resonance imaging which showed a solitary a 7 × 6 × 10 mm homogeneously contrast-enhancing lesion within the lumen of the posterior aspect of superior sagittal sinus without ventricular enlargement or peritumoral edema. The lesion was thought to be a meningioma radiographically. To evaluate the suspected increased intracranial pressure, a lumbar puncture was subsequently performed and demonstrated an opening pressure of 30 cm H2O. After drainage of 40 cc of CSF, the spinal closing pressure was 9 cm H2O. After failure of conservative management with acetazolamide, and determination of surgical inoperability due to the critical intraluminal location of the mass lesion, the patient underwent Gamma Knife radiosurgery. The 0.36 cc tumor was treated as an outpatient in the Perfexion® model Gamma Knife with a highly conformal and selective plan that enclosed the 3D geometry of the tumor with a minimal margin tumor dose of 14 gy at the 50% isodose. Three months after GKRS, the patient reported continued reduction in the frequency and severity of both her headaches and her visual disturbance. Ophthalmological consultation noted progressive resolution of her optic disc edema confirmed by formal optical coherence tomography. The patient is now 3 years out from GKRS with complete resolution of headache symptoms along with persistent reduction in tumor size (3 × 1 × 4 mm) on serial period imaging and resolution of papilledema.
Tumors located in such critical anatomic regions, as in our patient, should be considered for primary GKRS when the risks of biopsy or removal are too high. GKRS was able to provide great radiographic and clinical result in an intricately located meningioma.
伽玛刀立体定向放射外科手术(GKRS)可将辐射精确聚焦于颅内靶点,同时将周围正常组织的大量非靶点辐射降至最低。附着于或侵犯上矢状窦的脑膜瘤可能导致窦腔闭塞,且往往无法安全地完全切除。作者描述了一例位于上矢状窦后部完全内部的脑膜瘤患者的成功治疗。
一名46岁女性因进行性全身性头痛伴视力恶化就诊于急诊科。患者接受了脑部诊断性磁共振成像,显示在上矢状窦后部管腔内有一个7×6×10毫米的孤立性均匀强化病变,无脑室扩大或瘤周水肿。影像学上该病变被认为是脑膜瘤。为评估疑似升高的颅内压,随后进行了腰椎穿刺,测得初压为30厘米水柱。放出40毫升脑脊液后,脊髓终压为9厘米水柱。在使用乙酰唑胺保守治疗失败,且由于肿块病变位于管腔内的关键位置而确定无法进行手术切除后,患者接受了伽玛刀放射外科手术。在Perfexion®型伽玛刀中作为门诊患者对0.36立方厘米的肿瘤进行了治疗,采用了高度适形且选择性的计划,以50%等剂量线处最小边缘肿瘤剂量14戈瑞包围肿瘤的三维几何形状。GKRS术后三个月,患者报告头痛和视觉障碍的频率及严重程度持续减轻。眼科会诊指出,经正式光学相干断层扫描证实其视盘水肿逐渐消退。该患者目前已从GKRS手术中康复3年,头痛症状完全缓解,连续定期成像显示肿瘤大小持续缩小(3×1×4毫米),视乳头水肿消退。
对于像我们患者这样位于关键解剖区域的肿瘤,当活检或切除风险过高时,应考虑首选GKRS。GKRS能够为位置复杂的脑膜瘤提供良好的影像学和临床效果。