Department of Otolaryngology-Head and Neck Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
Department of Neurosurgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
PLoS One. 2021 Mar 26;16(3):e0248229. doi: 10.1371/journal.pone.0248229. eCollection 2021.
We describe the strategy used to repair intraoperative leaks of various grades and define factors for preventing postoperative cerebrospinal fluid leakage (CSF) after surgery via the endoscopic endonasal transsphenoidal approach (EETA).
Retrospective chart review at a tertiary referral center.
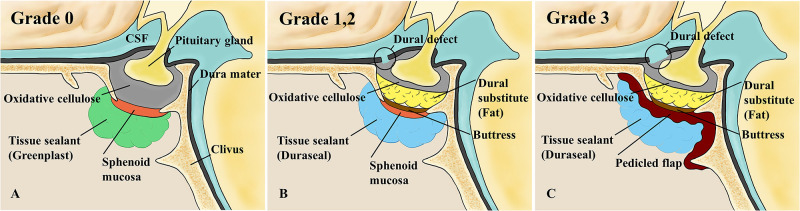
Patients who underwent surgery via EETA from January 2009 to May 2020 were retrospectively reviewed. Intraoperative CSF leakage was graded 0-3 in terms of the dural defect size; various repairs were used depending on the grade.
A total of 777 patients underwent 869 operations via EETA; 609 (70.1%) experienced no intraoperative CSF leakage (grade 0) but 260 (29.9%) did. Leakage was of grade 1 in 135 cases (15.5%), grade 2 in 83 (9.6%), and grade 3 in 42 (4.8%). In 260 patients with intraoperative CSF leakage, a buttress was wedged into the sellar defect site in 178 cases (68.5%) and a pedicled flap was placed in 105 cases (40.4%). Autologous fat (108 cases, 41.5%) and a synthetic dural substitute (91 cases, 35%) were used to fill the dead space of the sellar resection cavity. Postoperative CSF leakage developed in 21 patients: 6 of grade 1, 7 of grade 2, and 8 of grade 3. Buttress placement significantly decreased postoperative leakage in grade 1 patients (p = 0.041). In patients of perioperative leakage grades 2 and 3, postoperative CSF leakage was significantly reduced only when both fat and a buttress were applied (p = 0.042 and p = 0.043, respectively).
A buttress prevented postoperative CSF leakage in grade 1 patients; both fat and buttress were required by patients with intraoperative leakage of grades 2 and 3.
我们描述了一种策略,用于修复各种程度的术中渗漏,并确定通过内镜经鼻蝶入路(EETA)手术后预防术后脑脊液漏(CSF)的因素。
在三级转诊中心进行回顾性图表审查。
回顾性分析 2009 年 1 月至 2020 年 5 月期间接受 EETA 手术的患者。根据硬脑膜缺损大小,术中 CSF 渗漏分为 0-3 级;根据等级使用各种修复方法。
共有 777 例患者接受了 869 例 EETA 手术;609 例(70.1%)无术中 CSF 渗漏(0 级),但 260 例(29.9%)有。135 例(15.5%)为 1 级渗漏,83 例(9.6%)为 2 级渗漏,42 例(4.8%)为 3 级渗漏。在 260 例术中 CSF 渗漏患者中,178 例(68.5%)楔入鞍内缺陷部位,105 例(40.4%)放置带蒂皮瓣。自体脂肪(108 例,41.5%)和合成硬脑膜替代物(91 例,35%)用于填充鞍区切除腔的死腔。21 例患者术后出现 CSF 漏:1 级 6 例,2 级 7 例,3 级 8 例。放置支撑物可显著降低 1 级患者的术后渗漏(p = 0.041)。在术中漏级 2 和 3 的患者中,只有在应用脂肪和支撑物时,术后 CSF 漏才显著减少(分别为 p = 0.042 和 p = 0.043)。
支撑物可预防 1 级患者术后 CSF 渗漏;术中漏级 2 和 3 的患者需要脂肪和支撑物。