Li SiNi, Li JianHe, Peng LiuBao, Li YaMin, Wan XiaoMin
Clinical Nursing Teaching and Research Section, Second Xiangya Hospital, Central South University, Changsha, 410011, China.
Xiangya Nursing School, Central South University, Changsha, 410013, China.
Rheumatol Ther. 2021 Jun;8(2):775-791. doi: 10.1007/s40744-021-00300-4. Epub 2021 Mar 27.
A clinical trial (RACAT) reported the noninferiority of triple therapy compared to biologic agents (etanercept + methotrexate), and previous studies confirmed that biologic disease-modifying antirheumatic drugs (bDMARDs) are more expensive but less beneficial than triple therapy for patients with rheumatoid arthritis (RA) in whom methotrexate (MTX) fails. However, from the perspective of the Chinese healthcare system, the cost-effectiveness of triple therapy versus bDMARD treatment sequences as a first-line therapy for patients with RA is still unclear.
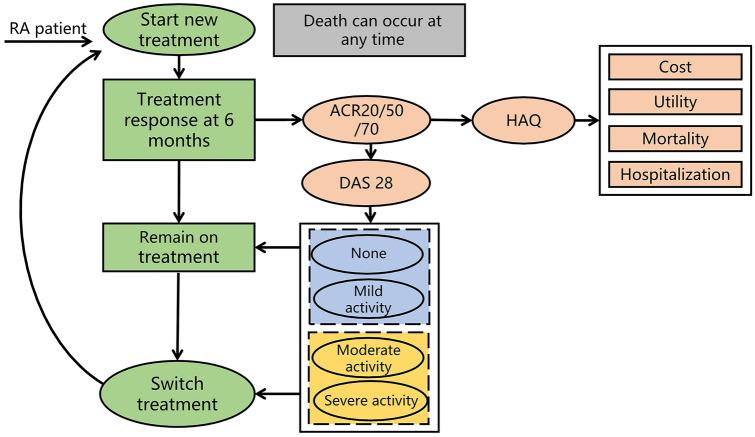
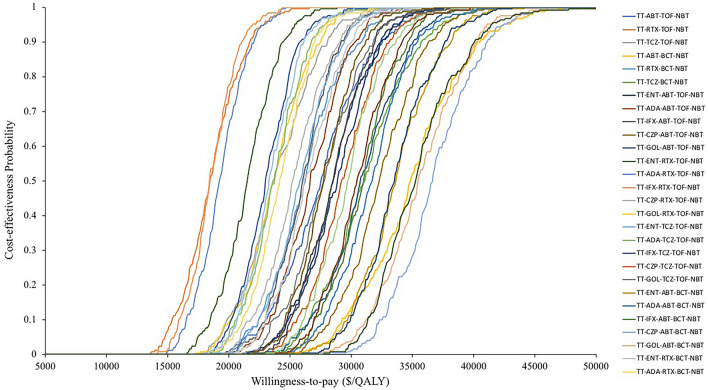
An individual patient simulation model was used to extrapolate the lifetime cost and health outcomes by tracing patients from initial treatment through switches to further treatment lines in a sequence. Therapeutic efficacy and physical function were evaluated using the American College of Rheumatology (ACR) response, 28-Joint Disease Activity Score (DAS28), and Health Assessment Questionnaire score. All input parameters in the model were derived from published studies, national databases, local hospitals, and experts' opinions. Both direct costs and indirect costs were taken into consideration. Probabilistic and one-way sensitivity analyses were performed to test the uncertainty of the model, as were multiple scenario analyses.
The lifetime analysis demonstrated that triple therapy was associated with lower costs and quality-adjusted life years (QALYs) than bDMARD sequences. These resulted in incremental cost-effectiveness ratios (ICERs) ranging from $87,090/QALY to $104,032/QALY, higher than the willingness-to-pay (WTP) threshold in China ($30,950/QALY). The baseline DAS28 impacted the model outcomes the most. Scenario analyses indicated that adding triple therapy to bDMARD sequences as a first-, second-, third-, or fourth-line therapy is very cost-effective, at a WTP of $10,316/QALY.
From a Chinese payer perspective, triple therapy as first-line treatment in treatment sequence could be regarded as cost-effectiveness option for patients who failed MTX, compared to bDMARDs as first-line treatment, and instead of prescribing triple therapy as a substitute for bDMARDs as a first-line treatment, adding triple therapy to the bDMARD treatment sequence is likely to be very cost-effective for patients with active RA compared to bDMARD sequences.
一项临床试验(RACAT)报告称,与生物制剂(依那西普+甲氨蝶呤)相比,三联疗法具有非劣效性,并且先前的研究证实,对于甲氨蝶呤(MTX)治疗失败的类风湿关节炎(RA)患者,生物性疾病改善抗风湿药物(bDMARDs)价格更高但益处更少。然而,从中国医疗体系的角度来看,三联疗法与bDMARD治疗方案作为RA患者一线治疗的成本效益仍不明确。
使用个体患者模拟模型,通过追踪患者从初始治疗到依次切换至后续治疗线的过程,推断其终身成本和健康结局。使用美国风湿病学会(ACR)反应、28关节疾病活动评分(DAS28)和健康评估问卷评分来评估治疗效果和身体功能。模型中的所有输入参数均来自已发表的研究、国家数据库、当地医院和专家意见。同时考虑了直接成本和间接成本。进行了概率分析和单因素敏感性分析以检验模型的不确定性,还进行了多种情景分析。
终身分析表明,与bDMARD治疗方案相比,三联疗法的成本和质量调整生命年(QALY)更低。这导致增量成本效益比(ICER)在87,090美元/QALY至104,032美元/QALY之间,高于中国的支付意愿(WTP)阈值(30,950美元/QALY)。基线DAS28对模型结果的影响最大。情景分析表明,在bDMARD治疗方案中添加三联疗法作为一线、二线、三线或四线治疗非常具有成本效益,支付意愿为10,316美元/QALY。
从中国支付方的角度来看,对于MTX治疗失败的患者,在治疗方案中将三联疗法作为一线治疗与将bDMARDs作为一线治疗相比,可被视为具有成本效益的选择,并且对于活动性RA患者,与bDMARD治疗方案相比,在bDMARD治疗方案中添加三联疗法可能非常具有成本效益,而不是将三联疗法作为bDMARDs一线治疗的替代方案。