Department of Andrology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 325000, Zhejiang, China.
School of Public Administration and Health, Wenzhou Medical University, Wenzhou, 325000, Zhejiang, China.
BMC Urol. 2021 Mar 27;21(1):48. doi: 10.1186/s12894-021-00817-4.
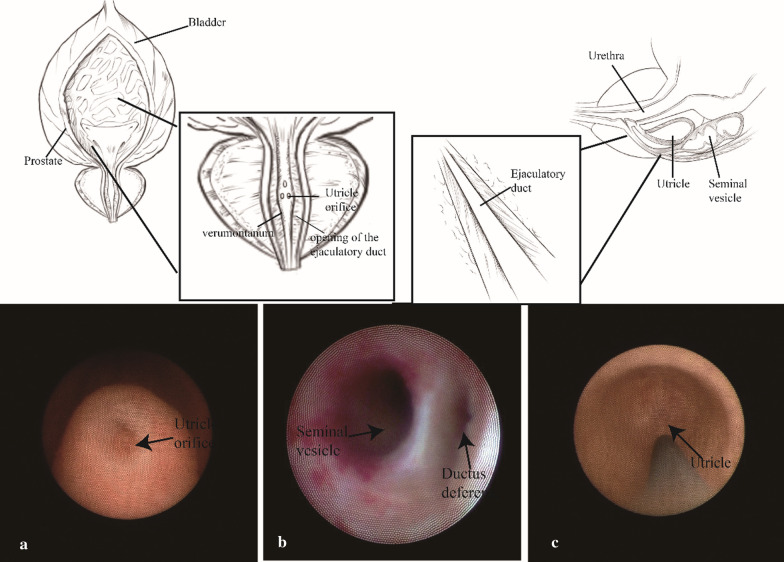
to describe the methodology of transurethral seminal vesiculoscopy and the anatomy of the area of the verumontanum, and to determine the safety of this procedure, especially in terms of postoperative complications.
This retrospective observational study enrolled 144 patients with intractable hematospermia from May 2011 and August 2019. A 4.5/6.5-Fr vesiculoscope was inserted into the seminal vesicle to deal with the positive findings. The solution of quinolones was used to rinse each seminal vesicle.
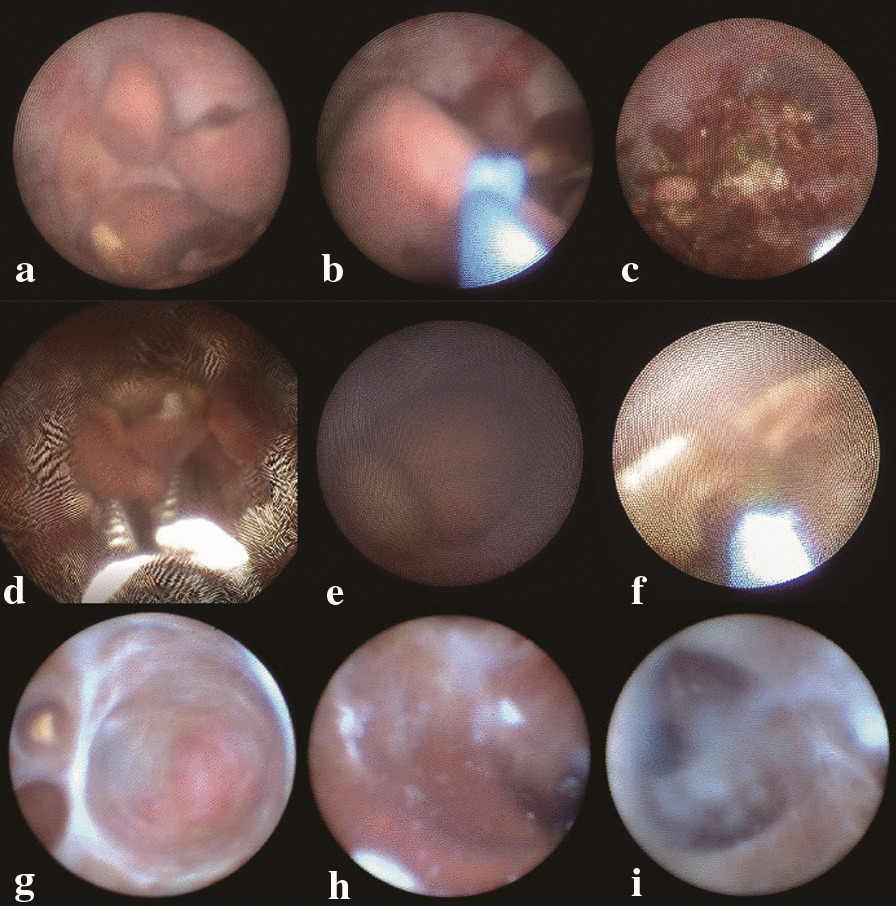
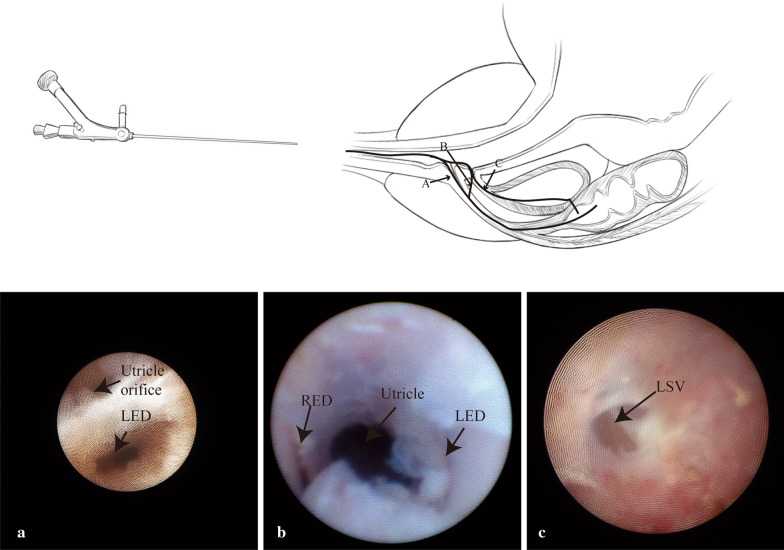
In this study, Transurethral seminal vesiculoscopy was successfully performed in 139 patients (96.53%). Hematospermia was alleviated or disappeared in 116 (80.56%) patients by less than half a year after surgery. Common intraoperative manifestations were hemorrhage, stones, utricle polyps and cysts. The surgical approach in our study were categorized into four types, including 24 (16.7%), 73 (50.7%), 42 (29.2%), and 5 (3.5%) cases in Type A (natural opening of the ejaculatory duct), B (trans-duct fenestration), C (trans-utricle fenestration), and D (not founded), respectively. Sexual function change was recorded in 12 patients of 111 patients, all by the method of trans-utricle fenestration, including 8 (7.21%), 3 (2.70%), and 1 (0.90%) patients in shorter intravaginal ejaculatory latency time, worse erection hardness and loss of orgasm, respectively.
Transurethral seminal vesiculoscopy is an effective and safe procedure for the management of hematospermia. The anatomy of the distal seminal tract should be understood more deeply and Wu'method (uncover-curtain method) needs to be promoted to verify its universality and safety. Besides, the complications of the function dysfunction should be discussed in the future in multi-center clinical trials.
描述经尿道精囊镜检查的方法学和舟状窝区域的解剖结构,并确定该手术的安全性,特别是在术后并发症方面。
本回顾性观察性研究纳入了 2011 年 5 月至 2019 年 8 月期间 144 例顽固性血精患者。将 4.5/6.5Fr 精囊镜插入精囊以处理阳性发现。使用喹诺酮溶液冲洗每个精囊。
在这项研究中,经尿道精囊镜检查在 139 例患者(96.53%)中成功进行。术后不到半年,116 例(80.56%)患者的血精减轻或消失。术中常见表现为出血、结石、舟状窝息肉和囊肿。我们的研究中的手术途径分为 4 种类型,A 型(射精管自然开口)24 例(16.7%),B 型(经管开窗)73 例(50.7%),C 型(经舟状窝开窗)42 例(29.2%),D 型(未发现)5 例(3.5%)。111 例患者中有 12 例记录到性功能改变,均采用经舟状窝开窗法,其中 8 例(7.21%)患者表现为阴道内射精潜伏期缩短,3 例(2.70%)患者勃起硬度变差,1 例(0.90%)患者射精快感缺失。
经尿道精囊镜检查是治疗血精症的一种有效且安全的方法。应更深入地了解远端精囊管的解剖结构,并推广 Wu 方法(揭幕法)以验证其普遍性和安全性。此外,未来应在多中心临床试验中讨论性功能障碍并发症的问题。