Schoeler Natasha E, Simpson Zoe, Zhou Runming, Pujar Suresh, Eltze Christin, Cross J H
Developmental Neurosciences Research and Teaching Department, University College London Great Ormond Street Institute of Child Health, London, United Kingdom.
Department of Dietetics, Great Ormond Street Hospital for Children, London, United Kingdom.
Front Neurol. 2021 Mar 12;12:643105. doi: 10.3389/fneur.2021.643105. eCollection 2021.
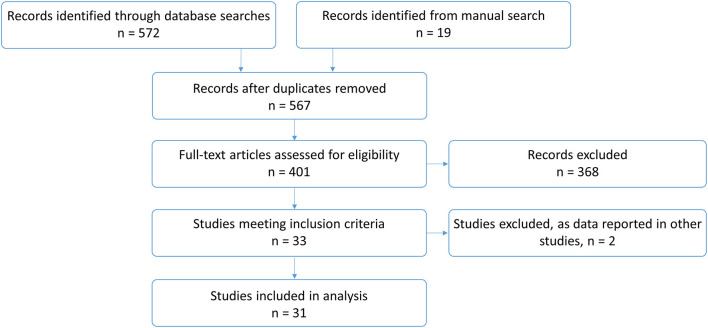
Ketogenic diet therapies (KDT) are high-fat, low carbohydrate diets used as an effective treatment option for drug-resistant epilepsy. There is limited research on the efficacy of KDT for super-refractory status epilepticus (SRSE). We systematically review evidence for use of KDT in children with SRSE and present a single UK tertiary centre's experience. Thirty one articles were included, of which 24 were "medium" or "low" quality. One hundred and forty seven children with SRSE started KDT, of which 141 (96%) achieved ketosis. KDT was started mean 5.3 days (range 1-420) after status epilepticus (SE) started. SRSE resolved in 85/141 (60%) children after mean 6.3 days (range 0-19) post SE onset, but it is unclear whether further treatments were initiated post-KDT. 13/141 (9%) children died. Response to KDT was more likely when initiated earlier ( = 0.03) and in females ( = 0.01). Adverse side effects were reported in 48/141 (34%), mostly gastrointestinal; potentially serious adverse effects occurred in ≤4%. Eight children with SRSE, all diagnosed with febrile infection-related epilepsy syndrome, were treated with KDT at Great Ormond Street Hospital for Children. KDT was initiated enterally at mean day 13.6+/- 5.1 of admission. Seven of 8 (88%) children reported adverse side effects, which were potentially serious in 4/8 (50%), including metabolic acidosis, hypoglycaemia and raised amylase. SE ceased in 6/8 (75%) children after mean 25+/- 9.4 days post onset, but other treatments were often started concomitantly and all children started other treatments post-KDT. Two of 8 (25%) children died during admission and another died post-admission. Four of the remaining 5 children continue to have drug-resistant seizures, one of whom remains on KDT; seizure burden was unknown for one child. Our findings indicate that KDT is possible and safe in children with SRSE. Cessation of SRSE may occur in almost two-thirds of children initiated with KDT, but a causal effect is difficult to determine due to concomitant treatments, treatments started post-KDT and the variable length of time post-KDT onset when SRSE cessation occurs. Given that serious adverse side effects seem rare and response rates are (cautiously) favorable, KDT should be considered as an early treatment option in this group.
生酮饮食疗法(KDT)是一种高脂肪、低碳水化合物的饮食,被用作耐药性癫痫的有效治疗选择。关于KDT治疗超难治性癫痫持续状态(SRSE)的疗效研究有限。我们系统回顾了KDT用于SRSE患儿的证据,并介绍了英国一家三级中心的经验。纳入了31篇文章,其中24篇质量为“中等”或“低等”。147名SRSE患儿开始接受KDT治疗,其中141名(96%)实现了酮症。KDT在癫痫持续状态(SE)开始后平均5.3天(范围1 - 420天)开始。141名患儿中有85名(60%)在SE发作后平均6.3天(范围0 - 19天)SRSE得到缓解,但尚不清楚KDT治疗后是否开始了进一步治疗。141名患儿中有13名(9%)死亡。KDT开始得越早(P = 0.03)以及女性(P = 0.01)对KDT的反应更可能较好。141名患儿中有48名(34%)报告了不良副作用,主要是胃肠道方面的;潜在严重不良副作用的发生率≤4%。大奥蒙德街儿童医院对8名SRSE患儿进行了KDT治疗,所有患儿均被诊断为发热感染相关癫痫综合征。KDT在入院平均第13.6±5.1天经肠道开始使用。8名患儿中有7名(88%)报告了不良副作用,其中4名(50%)可能较为严重,包括代谢性酸中毒、低血糖和淀粉酶升高。SE在发作后平均25±9.4天在6名(75%)患儿中停止,但其他治疗通常同时开始,且所有患儿在KDT治疗后都开始了其他治疗。8名患儿中有2名(25%)在住院期间死亡,另一名在出院后死亡。其余5名患儿中有4名继续有耐药性癫痫发作,其中一名仍在接受KDT治疗;一名患儿的癫痫发作负担未知。我们的研究结果表明,KDT对SRSE患儿是可行且安全的。接受KDT治疗的患儿中近三分之二的SRSE可能会停止,但由于同时进行的治疗、KDT治疗后开始的治疗以及SRSE停止时KDT开始后的时间长短不一,很难确定因果关系。鉴于严重不良副作用似乎罕见且缓解率(谨慎地)较为可观,KDT应被视为该组患儿的早期治疗选择。